Emergency Medical Minute
1,164 episodes — Page 5 of 24

Podcast 829: Monkeypox
Contributor: Aaron Lessen, MD Educational Pearls: Monkeypox transmission is still occurring in the United States Transmitted by contact to exposed lesion MSM are a high-risk group for monkeypox infection Symptoms include rash and flu like symptoms Monkeypox lesions are often described as blister-like, firm, clear, and rubbery Most commonly develop on the face and/or anogenital regions Patients with potential monkeypox infection should be moved to isolation to reduce risk of transmission Providers should use full PPE including N95, facial covering, gown, and gloves when interacting with a potential case of monkeypox Diagnosis involves swabbing the lesion and sending it for analysis People at risk for severe disease (i.e. immunocompromised) or who have severe symptoms (i.e. eye involvement) should begin treatment with Tecovirimat (TPOXX) in the ED Infectious Disease (ID) should be consulted, and the patient will need to follow up with ID regardless of symptom severity References Rizk JG, Lippi G, Henry BM, Forthal DN, Rizk Y. Prevention and Treatment of Monkeypox. Drugs. Jun 2022;82(9):957-963. doi:10.1007/s40265-022-01742-y Thornhill JP, Barkati S, Walmsley S, et al. Monkeypox Virus Infection in Humans across 16 Countries - April-June 2022. N Engl J Med. Aug 25 2022;387(8):679-691. doi:10.1056/NEJMoa2207323 Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD, & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/ Donate to EMM today!
Podcast 828: TXA Dosing Update
Contributor: Nick Hatch, MD Educational Pearls: In the setting of traumatic injury, tranexamic acid (TXA) is given to stabilize clots which minimizes bleeding and decreases risk of hemorrhagic shock Current TXA dose for trauma is 1 g bolus followed by a 1 g infusion; both doses should be given within 3 hours from time of injury Due to the split dose and narrow window, patients with complicated care, particularly if they require transfer may miss the infusion dose Various smaller studies have shown that dosing 2 g initially or 2 g followed by a 1 g infusion produces the same patient outcomes and no additional harm Receiving hospitals should strive to acquire accurate information regarding previous doses of TXA given and confirm timeline of injury References Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol Assess. 2013;17(10):1-79. doi:10.3310/hta17100 Ramirez RJ, Spinella PC, Bochicchio GV. Tranexamic Acid Update in Trauma. Crit Care Clin. 2017;33(1):85-99. doi:10.1016/j.ccc.2016.08.004 Spinella PC, Thomas KA, Turnbull IR, et al. The Immunologic Effect of Early Intravenous Two and Four Gram Bolus Dosing of Tranexamic Acid Compared to Placebo in Patients With Severe Traumatic Bleeding (TAMPITI): A Randomized, Double-Blind, Placebo-Controlled, Single-Center Trial. Front Immunol. 2020;11:2085. Published 2020 Sep 8. doi:10.3389/fimmu.2020.02085 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD, & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/ Donate to EMM today!

Podcast 827: Allergies in Peds
Contributor: Aaron Lessen, MD Educational Pearls: Recent study evaluated if early exposure to an allergen impacted the rate of allergy development later in childhood Children were exposed to peanut, milk, wheat, and egg allergens at 3 months of age and then followed for 3 years 2.5-3% of children who were not exposed developed allergies to these allergens 1% of children exposed to the allergens developed allergies to these allerrgens Exposing 63 children to allergens at 3 months would prevent the development of food allergy in one child with no significant adverse events Future recommendations will likely be to gradually introduce allergens to children starting around 3 months References Skjerven HO, Lie A, Vettukattil R, et al. Early food intervention and skin emollients to prevent food allergy in young children (PreventADALL): a factorial, multicentre, cluster-randomised trial. Lancet. Jun 25 2022;399(10344):2398-2411. doi:10.1016/s0140-6736(22)00687-0 Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD, & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/ Donate to EMM today!
Podcast 826: STEMI Equivalents
Contributor: Travis Barlock, MD Educational Pearls: The presence of a STEMI has traditionally been used to determine if a patient with acute chest pain requires urgent cath lab management STEMI indicates an occluded coronary artery, and urgent intervention is needed to restore perfusion to ischemic tissue Patients with occluded coronary arteries can present with EKG findings other than STEMI 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department was recently published in the Journal of the American College of Cardiology Recognizes STEMI equivalents that necessitate cath lab management ST depression in precordial leads Indicates a posterior infarct/possible RCA occlusion LBBB c ST elevation meeting modified Sgarbossa criteria Hyperacute and/or De Winter T wave First indication of coronary artery occlusion Most beneficial time to initiate cath lab because more tissue is salvageable These recommendations will likely alter clinical practice for ED management of acute chest pain References Kontos MC, de Lemos JA, Deitelzweig SB, et al. 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. Oct 6 2022;doi:10.1016/j.jacc.2022.08.750 Meyers HP, Bracey A, Lee D, et al. Comparison of the ST-Elevation Myocardial Infarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs. NOMI Paradigms of Acute MI. J Emerg Med. Mar 2021;60(3):273-284. doi:10.1016/j.jemermed.2020.10.026 Tziakas D, Chalikias G, Al-Lamee R, Kaski JC. Total coronary occlusion in non ST elevation myocardial infarction: Time to change our practice? Int J Cardiol. Apr 15 2021;329:1-8. doi:10.1016/j.ijcard.2020.12.082 Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD, & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/ Donate to EMM today!

Podcast 825: ALS vs PD Transport
Contributor: Aaron Lessen, MD Educational Pearls: In urban settings, it is becoming more common for police to transport critical patients from scene to hospital A 2022 multicenter observational study compared mortality rates in patients with penetrating injury to torso and/or proximal extremity when transported by EMS versus police Approximately 18% of patients were transported by police Overall mortality was approximately 15% in both groups In patients with more severe injury, mortality was still similar at approximately 36% and 38% respectively References Taghavi S, Maher Z, Goldberg AJ, et al. An analysis of police transport in an Eastern Association for the Surgery of Trauma multicenter trial examining prehospital procedures in penetrating trauma patients. J Trauma Acute Care Surg. 2022;93(2):265-272. doi:10.1097/TA.0000000000003563 Jacoby SF, Branas CC, Holena DN, Kaufman EJ. Beyond survival: the broader consequences of prehospital transport by police for penetrating trauma. Trauma Surg Acute Care Open. 2020;5(1):e000541. Published 2020 Nov 26. doi:10.1136/tsaco-2020-000541 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MS4 & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/ Donate to EMM today!
Podcast 824: Catheter-Related Blood Infections
Contributor: Travis Barlock, MD Educational Pearls: Catheter related blood infections were thought to be caused by skin flora seeding the catheter. Thus, significant effort is applied to sterility and skin preparation. However, studies have shown that bacteria growing on the tip of the catheter is not consistent with growth on cultures of skin. Staphylococcus epidermidis is commonly found on cultures of catheter sites. It has also been found in the gut flora of >50% of ICU patients. Rates of catheter related blood infections have been decreased through oral decontamination and early feeding. These findings suggest enteral bacterial translation as a major source of blood stream infection. References O'Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011;52(9):e162-e193. doi:10.1093/cid/cir257 von Eiff C, Becker K, Machka K, Stammer H, Peters G. Nasal carriage as a source of Staphylococcus aureus bacteremia. Study Group. N Engl J Med. 2001;344(1):11-16. doi:10.1056/NEJM200101043440102 ALTEMEIER WA, HUMMEL RP, HILL EO. Staphylococcal enterocolitis following antibiotic therapy. Ann Surg. 1963;157(6):847-858. doi:10.1097/00000658-196306000-00003 Marshall JC, Christou NV, Horn R, Meakins JL. The microbiology of multiple organ failure. The proximal gastrointestinal tract as an occult reservoir of pathogens. Arch Surg. 1988;123(3):309-315. doi:10.1001/archsurg.1988.01400270043006 Mrozek N, Lautrette A, Aumeran C, et al. Bloodstream infection after positive catheter cultures: what are the risks in the intensive care unit when catheters are routinely cultured on removal?. Crit Care Med. 2011;39(6):1301-1305. doi:10.1097/CCM.0b013e3182120190 Atela I, Coll P, Rello J, et al. Serial surveillance cultures of skin and catheter hub specimens from critically ill patients with central venous catheters: molecular epidemiology of infection and implications for clinical management and research. J Clin Microbiol. 1997;35(7):1784-1790. doi:10.1128/jcm.35.7.1784-1790.1997 Tani T, Hanasawa K, Endo Y, et al. Bacterial translocation as a cause of septic shock in humans: a report of two cases. Surg Today. 1997;27(5):447-449. doi:10.1007/BF02385710 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MS4 & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/ Donate to EMM today!
Podcast 823: Immediate Resuscitative Thoracotomy
Contributor: Jared Scott, MD Educational Pearls: Immediate resuscitative thoracotomy can be performed in the ED to gain rapid access to the thoracic cavity in cases of traumatic cardiac arrest Western Trauma Association Society Criteria for ED thoracotomy Blunt trauma + Penetrating trauma to torso + Penetrating trauma to the neck/extremity + Signs of life with refractory shock can consider resuscitative thoracotomy Outcomes in immediate resuscitative thoracotomy are poor but are improving A recent study evaluated over 2,000 patients meeting inclusion criteria for immediate resuscitative thoracotomy Overall survival rate of 20% 26% survival rate in penetrating trauma 7% survival rate in blunt trauma Predictors for poor outcomes Patient age > 60 years Blunt trauma mechanism of injury A prehospital or ED HR Absent signs of life at time of ED arrival When criteria are met, immediate resuscitative thoracotomy should rapidly be performed in the ED References Burlew CC, Moore EE, Moore FA, et al. Western Trauma Association critical decisions in trauma: resuscitative thoracotomy. J Trauma Acute Care Surg. 2012;73(6):1359-1363. Panossian VS, Nederpelt CJ, El Hechi MW, et al. Emergency Resuscitative Thoracotomy: A Nationwide Analysis of Outcomes and Predictors of Futility. J Surg Res. 2020;255:486-494. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MS4 & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/ Donate to EMM today!
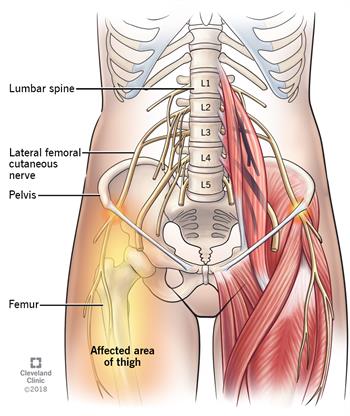
Podcast 822: Meralgia Paresthetica
Contributor: Aaron Lessen, MD Educational Pearls: Lateral Cutaneous Femoral Nerve Entrapment Syndrome, also known as Meralgia Paresthetica, results from entrapment of the lateral cutaneous femoral nerve, often as it exits the pelvis under the inguinal ligament. Meralgia Paresthetica is associated with obesity, pregnancy, compression from clothing or belts and diabetes. Symptoms include numbness, paresthesia and pain of the proximal lateral thigh. Signs or symptoms of radiculopathy such as weakness, loss of reflexes or severe back pain should not be present. Diagnosis is clinical and does not require further imaging if there are no additional or concerning findings. Meralgia Paresthetica typically resolves over time without intervention; however patients should be counseled on weight loss, diabetes control and avoidance of compressive clothing as relieving factors. References Solomons JNT, Sagir A, Yazdi C. Meralgia Paresthetica. Curr Pain Headache Rep. 2022;26(7):525-531. doi:10.1007/s11916-022-01053-7 Grossman MG, Ducey SA, Nadler SS, Levy AS. Meralgia paresthetica: diagnosis and treatment. J Am Acad Orthop Surg. 2001;9(5):336-344. doi:10.5435/00124635-200109000-00007 Image from my.clevelandclinic.org Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/ Donate to EMM today!
Podcast 821: EKGs in Syncope
Contributor: Travis Barlock, MD Educational Pearls: An EKG should be obtained quickly after a syncopal event to identify possible life-threatening causes such as ischemia and arrhythmia WOBBLER is a good mnemonic for remembering additional EKG findings to look for in syncope Wolff-Parkinson-White (WPW) Check for delta wave on QRS Obstructed AV node Any potential heart blocks Brugada syndrome Na channel blockade that can cause ST elevations in anterior leads Bifascicular block Conduction blockade in two of the three fascicles increases risk of complete heart block Left Ventricular Hypertrophy (LVH) Can be a sign of HOCM (younger patients) or aortic stenosis (older patients) Epsilon waves Positive deflections after the QRS that is seen in arrhythmogenic right ventricular dysplasia Repolarization abnormalities Prolonged/shortened QT segments References Martow E, Sandhu R. When Is Syncope Arrhythmic? Med Clin North Am. 2019;103(5):793-807. Solbiati M, Dipaola F, Villa P, et al. Predictive Accuracy of Electrocardiographic Monitoring of Patients With Syncope in the Emergency Department: The SyMoNE Multicenter Study. Acad Emerg Med. 2020;27(1):15-23. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/
Podcast 820: Who Qualifies for Take-Home Naloxone
Contributor: Don Stader, MD Educational Pearls: Home naloxone is traditionally given to those at high risk for opioid overdose such as those in the ED due to an opioid overdose, opioid intoxication, or admit to illicit opioid use There are a number of other patient populations that benefit from home naloxone including those on chronic opioid or benzodiazepine therapy, and those who report any type of illicit drug use Any illicit drug could be laced with opioids, and those who use drugs are more likely to be present as bystanders when an opioid overdose occurs Some important tips to remember when prescribing home naloxone There is often a scannable QR code that instructs bystanders on how to recognize and intervene in an overdose Inform the patient that naloxone is temporary and those who overdose are at high risk of overdosing again Provide support and inform the patient that if they decide they would like to enter treatment/rehabilitation programs, they can return to the ED to start that process References Strang J, McDonald R, Campbell G, et al. Take-Home Naloxone for the Emergency Interim Management of Opioid Overdose: The Public Health Application of an Emergency Medicine. Drugs. 2019;79(13):1395-1418. Moustaqim-Barrette A, Dhillon D, Ng J, et al. Take-home naloxone programs for suspected opioid overdose in community settings: a scoping umbrella review. BMC Public Health. 2021;21(1):597. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/ Donate to EMM today!
Podcast 819: Indiscriminate Lactate Testing
Contributor: Jared Scott, MD Educational Pearls: Elevated lactate levels can be a useful indicator of critical illness in patients who meet SIRS criteria Lactate can also be elevated due to other causes including seizures and medications such as albuterol and metformin A recent study from Switzerland* performed routine point-of-care lactate testing in all elderly patients presenting at triage in the emergency department in order to determine the prevalence of elevated lactate in the population and its utility in predicting poor patient outcomes Patients with seizure as their chief complaint were excluded from the study due to expected transient elevated lactate levels Poor outcomes were defined as requiring extensive IVF and/orvasoactive medications, undergoing intubation, admission to the ICU, or death 27.1% of patients had an increased lactate but only 7.3% actually met poor outcome criteria ED physicians should note that an increased lactate in an elderly patient does not mean that they are critically ill Routine point-of-care lactate monitoring at triage is of limited usefulness and should instead be targeted towards those who meet critical illness criteria *Errata: This study was performed in Switzerland, not Sweden as was stated in the podcast References Gosselin M, Mabire C, Pasquier M, et al. Prevalence and clinical significance of point of care elevated lactate at emergency admission in older patients: a prospective study. Intern Emerg Med. 2022;17(6):1803-1812. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/ Donate to EMM today!
Podcast 818: Local Anesthetics and LAST
Contributor: Don Stader, MD Educational Pearls: There are two major groups of local anesthetics: Amide and Esther To recall what group an anesthetic belongs to, use this memory trick: Amide has an 'i' in the name and Amide anesthetics have 2 'i's e.g., Lidocaine. Ester has no 'i' and most common Ester anesthetics have only one 'i' e.g., Tetracaine. In a true allergy and/or contraindication to both local anesthetic groups, diphenhydramine is an acceptable alternative. Epinephrine is administered with local anesthetics to decrease bleeding, increase duration of action, and minimize systemic spread of the anesthetic, thus reducing toxicity. Symptoms of Local Anesthetic Systemic Toxicity (LAST) may begin with dizziness, confusion and/or slurred speech, and can progress to cardiovascular collapse and death. Treat LAST with lipid emulsion therapy i.e. 'Intralipids' to create a lipid sink that absorbs anesthetic agent Administer initial 1.5 ml/kg bolus (approximately 100 ml in 70 mg adult) followed by infusion rate of 0.25 mg/kg/hour. Do not surpass 10 mg/kg total. References Dickerson DM, Apfelbaum JL. Local anesthetic systemic toxicity. Aesthet Surg J. 2014;34(7):1111-1119. doi:10.1177/1090820X14543102 Bina B, Hersh EV, Hilario M, Alvarez K, McLaughlin B. True Allergy to Amide Local Anesthetics: A Review and Case Presentation. Anesth Prog. 2018;65(2):119-123. doi:10.2344/anpr-65-03-06 Macfarlane AJR, Gitman M, Bornstein KJ, El-Boghdadly K, Weinberg G. Updates in our understanding of local anaesthetic systemic toxicity: a narrative review. Anaesthesia. 2021;76 Suppl 1:27-39. doi:10.1111/anae.15282 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz MD & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visithttps://emergencymedicalminute.com/edi-award/ Donate to EMM today!
Podcast 817: MI Risk during Elections
Contributor: Aaron Lessen, MD Educational Pearls: 2020 retrospective study with dat from two California hospitals compared rates of cardiovascular admissions in a five day period two weeks before and the five days after the presidential election Hospitalization rate for acute cardiovascular disease increased by 17% and rate of acute myocardial infarction increased by 42% Highest rates occurred in demographic of white males older than 75 years old No significant difference between groups in rates of stroke and heart failure References Mefford MT, Rana JS, Reynolds K, et al. Association of the 2020 US Presidential Election With Hospitalizations for Acute Cardiovascular Conditions. JAMA Netw Open. 2022;5(4):e228031. Published 2022 Apr 1. doi:10.1001/jamanetworkopen.2022.8031 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz MD & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/ Donate to EMM today!
Podcast 816: Ventilator Management in Asthmatics
Contributor: Aaron Lessen, MD Educational Pearls: The management of severe asthma or COPD exacerbation is complex, especially when the patient requires intubation/ventilation Asthma is an obstructive airway disease that can cause air trapping and hyperinflation of the lungs To avoid worsening hyperinflation patients typically require slower respiratory rates, lower tidal volumes, and increased expiratory time when on a ventilator Patients on a ventilator require very close monitoring to prevent worsening hyperinflation and associated complications including barotrauma and hypotension/cardiac arrest secondary to decreased venous return If patient condition starts to worsen, decrease respiratory rate and tidal volume In these cases, a decreased oxygen saturation is acceptable until their condition improves If patient status continues to worsen, consider disconnecting the ventilator and pushing on the chest for approximately 30 seconds to help force out trapped air If patient continues to decompensate, consider the possibility of a pneumothorax and determine if a chest tube is necessary Remember to continue asthma/COPD management including albuterol/duonebs, steroids, magnesium, and alternatives including as heliox References Demoule A, Brochard L, Dres M, et al. How to ventilate obstructive and asthmatic patients. Intensive Care Med. 2020;46(12):2436-2449 Garner O, Ramey JS, Hanania NA. Management of Life-Threatening Asthma: Severe Asthma Series. Chest. 2022 Laher AE, Buchanan SK. Mechanically Ventilating the Severe Asthmatic. J Intensive Care Med. 2018;33(9):491-501 Summarized by Mark O'Brien, MS4 | Edited by John Spartz MD & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/

Podcast 815: Fluid Resuscitation in Pancreatitis
Contributor: Aaron Lessen, MD Educational Pearls: Historically, pancreatitis has been treated with aggressive IV fluid rehydration. Recently published data shows this may not be appropriate. A randomized, controlled, multi-hospital trial evaluated outcomes for patients with acute pancreatitis receiving lactated Ringer's solution Aggressive fluid resuscitation group received 20ml/kg bolus + 3ml/hour Moderate fluid resuscitation groups received either 10 ml/kg bolus if hypovolemic or no bolus if normovolemic. Both moderate resuscitation groups received 1.5ml/hr. The primary outcome was development of moderately severe or severe pancreatitis. 22.1% of aggressive fluid resuscitation and 17.3% of moderate fluid resuscitation patients developed primary outcome. The safety outcome was fluid overload. Fluid overload developed in 20.5% of aggressive resuscitation group and only 6.3% of moderate resuscitation group. This trial was ended early due to differences in safety outcomes without obvious difference in primary outcome Overall, aggressive fluid resuscitation had no benefit in treatment of acute pancreatitis and providers should be aware of fluid overload risk. References de-Madaria E, Buxbaum JL, Maisonneuve P, et al. Aggressive or Moderate Fluid Resuscitation in Acute Pancreatitis. N Engl J Med. 2022;387(11):989-1000. doi:10.1056/NEJMoa2202884 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD In an effort to promote diversity, equity, and inclusion in Emergency Medicine, The Emergency Medical Minute is proud to present our 2nd annual Diversity and Inclusion Award. We support increasing the representation of underrepresented groups in medicine and extend this award to individuals applying to emergency medicine residencies during the 2022-2023 cycle. For information on award eligibility and the application process, visit https://emergencymedicalminute.com/edi-award/
Podcast 814: Post-concussion Treatment
Contributor: Aaron Lessen, MD Educational Pearls: Recent study looked at the impact of screen time on duration of post-concussive symptoms 125 patients aged 12-25 diagnosed with a concussion were randomized to either abstain from or have unrestricted screen time for 48 hours after injury Patients with unrestricted screen time averaged approximately 5 hours/day of screen time Patients in the no screen time group averaged approximately 1 hour/day of screen time Statistically significant difference in duration of post-concussive symptoms Unrestricted screen time cohort averaged 8 days of post-concussive symptoms No screen time cohort averaged 3.5 days of post-concussive symptoms ED physicians should encourage patients to limit screen time as much as possible in the first 48 hours after a concussion to promote faster recovery from post-concussive symptoms References Macnow T, Curran T, Tolliday C, et al. Effect of Screen Time on Recovery From Concussion: A Randomized Clinical Trial. JAMA Pediatr. 2021;175(11):1124-1131. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 813: Pulse Oximetry
Contributor: Travis Barlock, MD Educational Pearls: Most oxygen in the body is bound to hemoglobin, forming oxyhemoglobin. Less than 1% of the oxygen in the body is dissolved in plasma. Pulse Oximeters (Pulse Ox) function by emitting wavelengths of light from one side, and capturing the amount absorbed on the opposite side. A calculation determined the amount of saturation. Pulse Ox relies on pulsations in arterial flow to create a photoplethysmogram (pleth) for measurements Patients with poor peripheral perfusion may have unreliable pulse ox. Patient with an LVAD have constant flow and also unreliable pulse ox. Pulse Ox is a useful tool when pacing to determine mechanical capture. If there is disparity between the electrical wave pulse and the rate on pulse ox, there is likely no mechanical capture leading to poor distal flow. References Eecen CMW, Kooter AJJ. Pulsoximeters: werking, valkuilen en praktische tips [Pulse oximetry: principles, limitations and practical applications]. Ned Tijdschr Geneeskd. 2021;165:D5891. Published 2021 May 11. Elgendi M. On the analysis of fingertip photoplethysmogram signals. Curr Cardiol Rev. 2012;8(1):14-25. doi:10.2174/157340312801215782 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!

Podcast 812: PO Medications
Contributor: Nick Tsipis, MD Educational Pearls: PO medications are less frequently used in the ED due to their longer onset of action The position the patient is in when given PO medications may affect how quickly the medication is absorbed The quicker the medication passes through the stomach into the small intestine, the quicker it can be absorbed and metabolized Recent study used in silico gastric biomechanics model to compare the length of time it took PO medications to pass through the stomach based on the patient's positioning Compared the medication transit time in a stomach model placed in right lateral, left lateral, upright, and supine positions Right lateral positioning resulted in the fastest time for medication to pass through the stomach and enter the duodenum Likely due to the direction of gravity aligning with the antrum and pylorus of the stomach Left lateral positioning had the slowest time for the pill to enter the small intestine Likely due to gravity not aligning with stomach anatomy The time to absorption in the right and left lateral position were significantly faster and slower respectively than that seen in the upright and supine positions These results indicate that placing a patient in the right lateral position when giving PO medications may result in faster rate of medication onset than if the patient is in another position References Lee JH, Kuhar S, Seo JH, Pasricha PJ, Mittal R. Computational modeling of drug dissolution in the human stomach: Effects of posture and gastroparesis on drug bioavailability. Phys Fluids (1994). 2022;34(8):081904. Summarized by Mark O'Brien, MS4 | Edited by John Spartz MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 811: Ketamine for Pain
Contributor: Lessen, Aaron MD Educational Pearls: Ketamine can be given at 0.2-0.3 mg/kg as subdissociative doses for pain control in the ED Ketamine coadministered with Haldol may reduce agitation A recent study in Iran compared subdissociative Ketamine given with 2.5 mg Haldol to 1 mg/kg Fentanyl for pain control in the ED Ketamine with Haldol had better pain control than Fentanyl at 5, 10, 15 and 30 minutes Ketamine with Haldol less frequently required rescue medication Ketamine with Haldol did have increased agitation at only the 10 minute mark Of note, there was not a Ketamine only group to compare Ketamine with Haldol is a viable alternative combination for pain control References Moradi MM, Moradi MM, Safaie A, Baratloo A, Payandemehr P. Sub dissociative dose of ketamine with haloperidol versus fentanyl on pain reduction in patients with acute pain in the emergency department; a randomized clinical trial. Am J Emerg Med. 2022;54:165-171. doi:10.1016/j.ajem.2022.02.012 Sin B, Ternas T, Motov SM. The use of subdissociative-dose ketamine for acute pain in the emergency department. Acad Emerg Med. 2015;22(3):251-257. doi:10.1111/acem.12604 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!

Podcast 810: Tooth Replantation
Contributor: Jarod Scott, MD Educational Pearls: There is a 1-hour window for tooth replantation in ED Cold milk is often best transport media unless there is access to specialized solutions (Hank's Balanced Solution) Goal is to preserve periodontal ligament Soaking in tap water should be avoided as it will lyse cells of periodontal ligament If oral surgeon is rapidly available, have them perform replantation Do not delay replantation to wait for an oral surgeon to become available Steps in tooth reimplantation Disturb the socket as little as possible Handle tooth only by crown, don't touch root Rinse tooth gently with tap water or saline, do not scrub it Tooth should click back in place and remain stable Don't manipulate after reimplantation It may take weeks to determine if the tooth will survive Studies have shown that replantation performed within one hour has a significantly better prognosis than those taking place after a greater amount of time has passed References Alotaibi S, Haftel A, Wagner ND. Avulsed Tooth. In: StatPearls. Treasure Island (FL): StatPearls Publishing. Copyright © 2022, StatPearls Publishing LLC.; 2022. Andreasen JO, Andreasen FM, Skeie A, Hjørting-Hansen E, Schwartz O. Effect of treatment delay upon pulp and periodontal healing of traumatic dental injuries – a review article. Dent Traumatol. 2002;18(3):116-128. De Brier N, O D, Borra V, Singletary EM, Zideman DA, De Buck E. Storage of an avulsed tooth prior to replantation: A systematic review and meta-analysis. Dent Traumatol. 2020;36(5):453-476. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
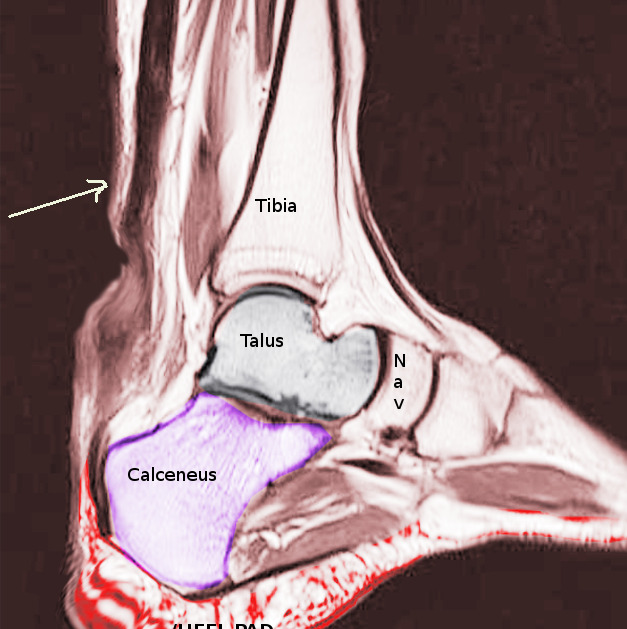
Podcast 809: Achilles Tendon Rupture
Contributor: Aaron Lessen, MD Educational Pearls: Achilles tendon rupture usually presents in younger, healthy patients after a sports injury Patients typically present complaining of an abrupt onset ankle pain after feeling a "pop" Pain can be localized to posterior ankle and patient's lack the ability to plantarflex Achilles rupture is a clinical diagnosis and does not usually require imaging in the ED Thompson test Having patient lay on their stomach and squeezing the calf on the injured side should result in plantarflexion If the Achilles is ruptured, no plantarflexion will occur Treatment in the ED is to place the patient in a short leg posterior splint with some mild plantarflexion to aid in healing After discharge patients should follow up with orthopedics Recent study compared those who underwent the traditional open surgery, a minimally invasive surgery, and no surgery No difference in functionality was noted between the groups 3 months to 1 year post injury Those in the nonoperative group had slightly higher rates of repeat rupture (6%) than those in the surgical groups ( Patients undergoing minimally invasive surgery had the highest risk of nerve injury (5.2%), followed by traditional surgery (2.8%), and then nonoperative (0.6%) References Cuttica DJ, Hyer CF, Berlet GC. Intraoperative value of the thompson test. J Foot Ankle Surg. 2015;54(1):99-101. Kauwe M. Acute Achilles Tendon Rupture: Clinical Evaluation, Conservative Management, and Early Active Rehabilitation. Clin Podiatr Med Surg. 2017;34(2):229-243. Myhrvold SB, Brouwer EF, Andresen TKM, et al. Nonoperative or Surgical Treatment of Acute Achilles' Tendon Rupture. N Engl J Med. 2022;386(15):1409-1420. Summarized by Mark O'Brien, MS4 | Edited by John Spartz MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 808: BVM and PEEP Valve
Contributor: Dylan Luyten, MD Educational Pearls: Positive End Expiratory Pressure (PEEP) is positive pressure within the lungs and maintained throughout the entire respiratory cycle. It is the pressure preventing alveoli from collapsing at the end of exhalation. When using a bag valve mask (BVM) to ventilate patients, always attach the PEEP valve to prevent intrathoracic pressure from returning to atmospheric pressure which would allow alveoli collapse. A BVM with a good seal to patients face and with an attached PEEP valve provides the same support as BiPAP or CPAP. A generally acceptable PEEP setting is 5 cmH2O. References Mora Carpio AL, Mora JI. Positive End-Expiratory Pressure. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 27, 2021. Harrison MJ. PEEP and CPAP. Br Med J (Clin Res Ed). 1986;292(6521):643-644. doi:10.1136/bmj.292.6521.643 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 807: Ring Removal Tricks
Contributor: Jared Scott, MD Educational Pearls: If a patient is in significant pain, a digital block can be helpful. Pain management alone may allow for manual ring removal. Ring cutters and trauma shears with specialized ring cutters can be attempted but will destroy the ring and some materials may be resistant to cutting. 2 alternative options are presented which aim to reduce edema above the ring to assist removal: Move the ring as proximally as possible. Wrap large size suture from the ring distally beyond PIP joint. Slide the ring over the suture and off the finger. Wrap a tourniquet from distal to proximal including over the ring. Have the patient hold the tourniquet in place while they elevate their hand above the head for 15 minutes. Take down the tourniquet then remove the ring. References Asher CM, Fleet M, Bystrzonowski N. Ring removal: an illustrated summary of the literature. Eur J Emerg Med. 2020;27(4):268-273. doi:10.1097/MEJ.0000000000000658 Walter J, DeBoer M, Koops J, Hamel LL, Rupp PE, Westgard BC. Quick cuts: A comparative study of two tools for ring tourniquet removal. Am J Emerg Med. 2021;46:238-240. doi:10.1016/j.ajem.2020.07.039 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!

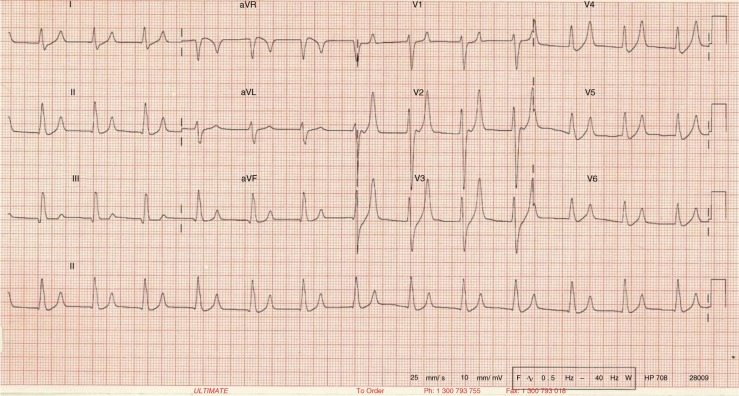
Podcast 806: Normal ECGs
Contributor: Jared Scott, MD Educational Pearls: Physicians are typically advised not to trust computer interpretation of ECGs Retrospective study was done of computer interpreted normal ECGs to evaluate the accuracy of such an interpretation 989 ECGs were interpreted as "Normal sinus rhythm, Normal ECG" by proprietary cardiology software on MUSE Cardiology Information System These EKGs received follow up interpretation by cardiologists which was considered the "gold standard" for interpretation 18.6% of "normal ECG" had at least one abnormality identified by the cardiologist 6.1% of these discrepant interpretations were deemed potentially clinically significant Only 1% were classified as possible ischemia On retrospective chart review: Six patients underwent non-emergent cardiac catheterization Two had cardiac interventions One had three PCI stents to a prior CABG graft One had a scheduled outpatient cardiac catheterization but was admitted and ended up receiving a CABG graft Study showed that discrepancies between computer interpretation of "Normal ECG" and cardiologist re-interpretation were not clinically significant Emergency physicians should still screen ECGs per AHA guidelines References Winters LJ, Dhillon RK, Pannu GK, Terrassa P, Holmes JF, Bing ML. Emergent cardiac outcomes in patients with normal electrocardiograms in the emergency department. Am J Emerg Med. 2022;51:384-387. Summarized by Mark O'Brien, MS4 | Edited by John Spartz MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 805: Tunneled Peritoneal Catheter
Contributor: Aaron Lessen, MD Educational Pearls: Patients with recurrent ascites may need frequent outpatient or emergency department paracentesis which can be time consuming and uncomfortable for patients. Tunneled peritoneal catheters are a permanent alternative therapy which allows fluid drainage at home by patient or caregiver. There has been theoretical concern that long term placement of tunneled peritoneal catheters may increase risk of infection, thus they are more commonly placed as a palliative measure for patients with end stage cancer and malignant ascites with shorter anticipated life spans. However, a recent small study found that in both patients with malignant ascites and recurrent ascites from cirrhosis, tunneled peritoneal catheter placement reduced symptoms from ascites and did not increase risk of infection or leakage at catheter site, or spontaneous bacterial peritonitis after four weeks. More research is emerging and tunneled peritoneal catheters may become more common. References Kimer N, Riedel AN, Hobolth L, et al. Tunneled Peritoneal Catheter for Refractory Ascites in Cirrhosis: A Randomized Case-Series. Medicina (Kaunas). 2020;56(11):565. Published 2020 Oct 27. doi:10.3390/medicina56110565Petzold G, Bremer SCB, Heuschert FC, et al. Tunnelled Peritoneal Catheter for Malignant Ascites-An Open-Label, Prospective, Observational Trial. Cancers (Basel). 2021;13(12):2926. Published 2021 Jun 11. doi:10.3390/cancers13122926Corrigan M, Thomas R, McDonagh J, et al. Tunnelled peritoneal drainage catheter placement for the palliative management of refractory ascites in patients with liver cirrhosis. Frontline Gastroenterol. 2020;12(2):108-112. Published 2020 Feb 28. doi:10.1136/flgastro-2019-101332 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
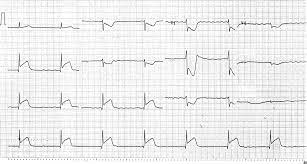
Podcast 804: Brugada Criteria for V Tach
Contributor: Peter Bakes, MD Educational Pearls: Tachycardia describes a heart rate of >120 beats per minute Wide Complex describes a QRS duration of >120 ms or 3 small boxes on a standard EKG The major differential for a wide complex tachycardia is Ventricular Tachycardia (VT), aka "V Tach", or Supraventricular Tachycardia (SVT) with Aberrancy SVT alone is a narrow complex tachycardia, but as rate increases a right or left bundle branch block pattern may emerge, creating SVT with Aberrancy seen as a wide complex on EKG It is important to distinguish the rhythms as treatment for stable VT differs from treatment(s) for stable SVT Brugada Criteria is an algorithm for determining if wide complex tachycardia is VT with a high degree of sensitivity and specificity. Following is a simple ED approach based on brugada criteria to determine VT on EKG. If either condition is true, suspect and treat VT: Concordance: All precordial leads have QRS complexes that are either all positive or all negative. R-S interval: >100 ms in any one precordial lead. Also note that VT is more common in patients who are elderly and/or have cardiac comorbidities of ischemic or structural heart disease References Reithmann C. Tachykardien mit breiten QRS-Komplexen [Differential diagnosis of wide QRS complex tachycardia]. MMW Fortschr Med. 2019;161(13):48-56. doi:10.1007/s15006-019-0022-x Ding WY, Mahida S. Wide complex tachycardia: differentiating ventricular tachycardia from supraventricular tachycardia. Heart. 2021;107(24):1995-2003. doi:10.1136/heartjnl-2020-316874 Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation. 1991;83(5):1649-1659. doi:10.1161/01.cir.83.5.1649 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 803: Sedation During Intubation
Contributor: Aaron Lessen, MD Educational Pearls: Awareness with recall of paralysis can occur in intubated and ventilated patients receiving paralytic medications Patients who suffer from this effect are at high risk of developing severe PTSD, depression, and suicidal ideations Occurs in approximately 0.1-0.2% of patients undergoing general anesthesia in an OR setting 2021 study showed patients intubated in the ED have a much higher rate of experiencing awareness during intubation 2.6% chance of awareness in patients undergoing intubation and mechanical ventilation in the ED Higher rates with rocuronium likely due to its longer duration of action New follow up study from 2022 showed 3.4% of patients aware when paralyzed for mechanical ventilation in ED 5.5% of patients receiving rocuronium had awareness occur Patients who received other paralytics had a Important to be proactive with sedation and pain medications to decrease risk of awareness with recall of paralysis, especially in patients receiving rocuronium References Fuller BM, Pappal RD, Mohr NM, et al. Awareness With Paralysis Among Critically Ill Emergency Department Patients: A Prospective Cohort Study. Crit Care Med. 2022. Leslie K, Davidson AJ. Awareness during anesthesia: a problem without solutions? Minerva Anestesiol. 2010;76(8):624-628. Pappal RD, Roberts BW, Mohr NM, et al. The ED-AWARENESS Study: A Prospective, Observational Cohort Study of Awareness With Paralysis in Mechanically Ventilated Patients Admitted From the Emergency Department. Ann Emerg Med. 2021;77(5):532-544. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Pediatric Palliative Care Expert Panel
Selected audio from our event, Palliative, hosted on June 27, 2022 in conjunction with Children's Hospital Colorado's Department of Palliative Medicine and The Denver Hospice's Footprints Program. Keynote address by Dr. Nadia Tremonti, pediatric palliative care physician at Children's Hospital of Michigan Expert Panel composed of Dr. Kimberly Bennett, medical director for TDH's Footprints Program, Dora Mueller, clinical nurse coordinator for palliative care at Children's and Cassie Matz, LCSW bereavement coordinator at Children's. The evening commenced following a screening of the 2019 award-winning documentary, Palliative, featuring Dr. Nadia Tremonti's work at Children's Hospital of Michigan. You can watch the documentary for free at Kanopy.com using your library card using the following link: https://www.kanopy.com/product/palliative
Podcast 802: Intranasal Medication Administration for Pediatric Patients
Contributor: Aaron Lessen, MD Educational Pearls: Intranasal medication administration is a convenient, quick, and relatively painless option for pediatric patients Often used as an initial medication to help control pain in children prior to establishing an IV Using an atomizer is preferred when administering intranasal medications The syringe should be angled towards the ipsilateral eye or occiput rather than straight upwards Do not administer more than 1 mL of fluid per nostril as volumes greater than 1 mL are not sufficiently absorbed Intranasal medication doses differ from the traditional IV dosages and have a slower onset of action References Del Pizzo J, Callahan JM. Intranasal medications in pediatric emergency medicine. Pediatr Emerg Care. 2014;30(7):496-501; quiz 502-494. Fantacci C, Fabrizio GC, Ferrara P, Franceschi F, Chiaretti A. Intranasal drug administration for procedural sedation in children admitted to pediatric Emergency Room. Eur Rev Med Pharmacol Sci. 2018;22(1):217-222. Rech MA, Barbas B, Chaney W, Greenhalgh E, Turck C. When to Pick the Nose: Out-of-Hospital and Emergency Department Intranasal Administration of Medications. Ann Emerg Med. 2017;70(2):203-211. Schoolman-Anderson K, Lane RD, Schunk JE, Mecham N, Thomas R, Adelgais K. Pediatric emergency department triage-based pain guideline utilizing intranasal fentanyl: Effect of implementation. Am J Emerg Med. 2018;36(9):1603-1607. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Mental Health Monthly #14: Substance-Induced Psychosis (Part II)
In this second episode of a two-part mini-series, we feature Dr. Nadia Haddad, a Colorado psychiatrist, and Dr. Ricky Dhaliwal, an emergency medicine physician, as they discuss the various treatment modalities for substance-induced psychosis. They explore pharmacologic treatments, inpatient and outpatient treatments, and ways that emergency providers can improve their care for psychiatric patients with comorbid medical conditions. Lastly, they consider the different causes for repeat visits from mentally ill patients. Key Points: Pharmacologic treatments for substance-induced psychosis are similar to those for other types of psychosis; these include medications like Zyprexa, Haldol, and, as a third-line treatment, IM Thorazine. Droperidol is used more commonly in the emergency setting, compared with the psychiatric setting. Given the risk for respiratory depression from Zyprexa combined with benzodiazepines, psychiatrists may choose to use Thorazine or Haldol/Ativan/Benadryl instead. It is important to reassess patients after substances wear off to determine whether they meet criteria for admission to inpatient psychiatry, though psychiatric assessments are limited by geographic constraints. The admitting psychiatry team will reassess the patient to differentiate substance-induced psychosis vs other psychoses; often this includes obtaining collateral. Helpful notes from the ED include: medications administered or restraints placed (can help extrapolate a patient's level of agitation), vital signs, prior records. Some people will be more open about suicidality while intoxicated and less open about it while sober so it is important to obtain additional information for corroboration. On average, patients stay in the detox unit for 3-4 days, though some may stay longer for protracted substance-induced psychosis if they have a long-standing history of daily substance use. It is important to discharge patients with quick follow-up and potential placement into the various mental health programs including partial hospitalization, residential, or outpatient programs. Emergency rooms can improve by taking psychiatric patients seriously, especially when they are transferred to the hospital from a psychiatric facility for medical management. Repeat visits stem partially from the ambivalence that accompanies substance use disorders, including patients' difficulty in giving up the substance due the purpose it may serve in their lives. Many substance use disorder programs are siloed from the medical system, which pose a challenge to interdisciplinary communication.
Podcast 801: Push Dose Vasopressors
Contributor: Aaron Lessen, MD Educational Pearls: There are two common options for push-dose vasopressor: phenylephrine and epinephrine. Both have been studied in the setting of the OR, but are lacking data in emergency room utilization. A recent retrospective study at one hospital compared the two options for effectiveness and safety. The data showed phenylephrine raised systolic pressure an average 26 points while epinephrine raised the systolic pressure higher, an average of 33 points. Additionally, the same study showed dosing errors were more common in epinephrine. The error rates were 13% and 2% when using premixed syringes of epinephrine and phenylephrine respectively. However, overall no increase in adverse outcomes were reported between the two drugs in this study. References Nam E, Fitter S, Moussavi K. Comparison of push-dose phenylephrine and epinephrine in the emergency department. Am J Emerg Med. 2022;52:43-49. doi:10.1016/j.ajem.2021.11.033 Weingart S. Push-dose pressors for immediate blood pressure control. Clin Exp Emerg Med. 2015;2(2):131-132. Published 2015 Jun 30. doi:10.15441/ceem.15.010 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!

Podcast 800: Mortality in Fevers
Contributor: Aaron Lessen, MD Educational Pearls: A recent study evaluated the association between the degree of fever and mortality rate in patients presenting to a set of Emergency Departments in Israel Febrile patients with a temperature > 38.0 C were recorded and these patients were compared against local death records to determine the all-cause 30-day mortality rate 8.1% of patients evaluated in the ED were determined to be febrile 30-day mortality for all febrile patients was around 12% Patients with fever >40 C have a mortality rate approaching 24% Patients febrile to >40 C had increased mortality, ICU admissions, and AKIs compared to those with lesser degrees of fever Those with a body temperature of between 39.2-39.5 C had the lowest mortality rates which may indicate the protective role of fever and warrants further research References Marcusohn E, Gibory I, Miller A, Lipsky AM, Neuberger A, Epstein D. The association between the degree of fever as measured in the emergency department and clinical outcomes of hospitalized adult patients. Am J Emerg Med. 2022;52:92-98. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
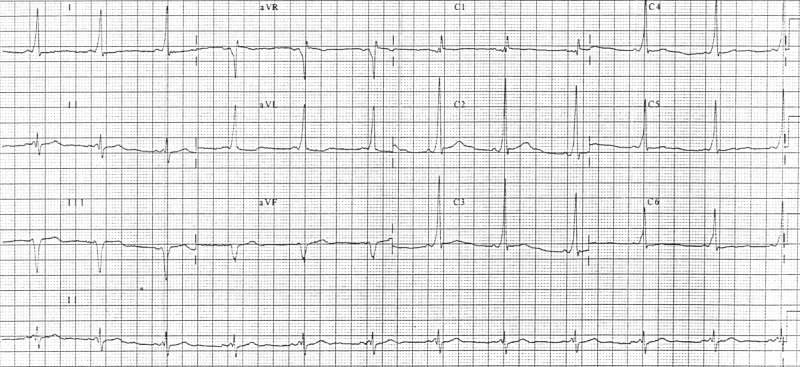
Podcast 799: EKG Abnormalities in Renal Failure
Contributor: Peter Bakes, MD Educational Pearls: Patients in renal failure may have elevated serum potassium levels which can result in EKG changes. EKG changes in the setting of hyperkalemia generally depend on the serum level. Mild elevation may cause peaked T waves. At higher serum levels there will be loss of P waves plus wide complex tachycardia. There can be progression to fatal arrhythmias. Treatment of acute hyperkalemia involves multiple mechanisms. Calcium gluconate stabilizes the cardiac membrane (of note, its duration of action is 1 hour). Insulin with Glucose and Bicarbonate both act to shift extracellular potassium into cells. Enhanced elimination of potassium is accomplished via Kayexalate or Lokelma. Definitive treatment for hyperkalemia is hemodialysis. The differential for wide complex non-tachycardic rhythm on EKG includes: left ventricular hypertrophy, left bundle branch block, pacemaker, electrolyte abnormalities including hyperkalemia. References Palmer BF, Clegg DJ. Diagnosis and treatment of hyperkalemia. Cleve Clin J Med. 2017;84(12):934-942. doi:10.3949/ccjm.84a.17056 Watanabe R. Hyperkalemia in chronic kidney disease. Rev Assoc Med Bras (1992). 2020;66Suppl 1(Suppl 1):s31-s36. Published 2020 Jan 13. doi:10.1590/1806-9282.66.S1.31 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 797: Vitamin C in Sepsis
Contributor: Aaron Lessen, MD Educational Pearls: Prior, smaller studies showed intravenous Vitamin C given to patients with sepsis significantly improved patient mortality and additional outcomes. A recently published, randomized control trial with >800 ICU patients who received up to 4 days of IV Vit C or placebo concluded that the end points of death or persistent organ dysfunction at 28 days were unaffected by Vitamin C administration. There were no adverse safety outcomes associated with Vitamin C administration. Based on this trial, it is unlikely that Vitamin C will become a mainstay of treatment for sepsis patients. References Marik PE, Khangoora V, Rivera R, Hooper MH, Catravas J. Hydrocortisone, Vitamin C, and Thiamine for the Treatment of Severe Sepsis and Septic Shock: A Retrospective Before-After Study. Chest. 2017;151(6):1229-1238. doi:10.1016/j.chest.2016.11.036 Lamontagne F, Masse MH, Menard J, et al. Intravenous Vitamin C in Adults with Sepsis in the Intensive Care Unit. N Engl J Med. 2022;386(25):2387-2398. doi:10.1056/NEJMoa2200644 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!

Podcast 796: Fluid Amounts in Septic Shock
Contributor: Aaron Lessen, MD Educational Pearls: Septic shock management has traditionally endorsed rapid fluid resuscitation and the administration of vasopressors Current guidelines are for patients to initially receive a 30 ml/kg fluid bolus then additional fluid as needed for continued hypotension The ideal volume of fluid needed to maximize patient outcomes has been debated A recent ICU-based study examined mortality differences between patient receiving restricted vs standard fluid therapy for septic shock There was no significant difference in the rate of mortality or adverse outcomes between the two groups indicating that the amount of fluid used after the initial bolus does not affect patient outcomes More research needed to evaluate the ideal fluid volumes used in the initial resuscitation of septic shock Errata: *** "The primary outcome was death within 90 days after randomization" References Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181-1247. Meyhoff TS, Møller MH, Hjortrup PB, Cronhjort M, Perner A, Wetterslev J. Lower vs higher fluid volumes during initial management of sepsis: a systematic review with meta-analysis and trial sequential analysis. Chest. 2020;157(6):1478-1496. Meyhoff TS, Hjortrup PB, Wetterslev J, et al. Restriction of Intravenous Fluid in ICU Patients with Septic Shock. N Engl J Med. 2022;386(26):2459-2470. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 795: Lithium Toxicity
Contributor: Peter Bakes, MD Educational Pearls: Lithium remains a commonly used medication for treating bipolar disorder Lithium toxicity can be acute, acute-on-chronic, or chronic Measuring blood lithium level Therapeutic range of lithium is around 1.6-1.8 mEq/L >2 mEq/L is likely to cause significant toxicity >4 mEq/L necessitates lifesaving treatment The lethal dose of lithium is 700 mg/kg Lithium can have delayed absorption resulting in levels increasing during hospitalization Symptoms associated with acute lithium toxicity Gastrointestinal Nausea, vomiting, abdominal pain Neurological Tremor, nystagmus, CNS depression (late finding) Cardiovascular Bradycardia, QT prolongation, EKG changes Treatment for lithium toxicity ABCs Get a good history GI Decontamination: Whole bowel irrigation if patient ingested extended-release tablets Dialysis Most effective treatment for lithium toxicity References Baird-Gunning J, Lea-Henry T, Hoegberg LCG, Gosselin S, Roberts DM. Lithium Poisoning. J Intensive Care Med. 2017;32(4):249-263. Hedya SA, Avula A, Swoboda HD. Lithium Toxicity. In: StatPearls. Treasure Island (FL): StatPearls Publishing. Copyright © 2022, StatPearls Publishing LLC.; 2022. McKnight RF, Adida M, Budge K, Stockton S, Goodwin GM, Geddes JR. Lithium toxicity profile: a systematic review and meta-analysis. Lancet. 2012;379(9817):721-728. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 793: Postintubation Sedation and Analgesia
Contributor: Peter Bakes, MD Educational Pearls: When intubating a patient, it is important to consider what medications will be used for post-intubation sedation and analgesia The common non-benzodiazepine sedating medications are propofol, precedex, and ketamine Propofol is frequently used in the emergency department, and it lowers ICP and MAP making it the preferred sedative for patients with intracranial bleeds Precedex is a milder sedative used in the ICU because it decreases time to extubation and reduces the risk of complications associated with long term intubation Ketamine should be used in hypotensive patients because it does not lower blood pressure, and its bronchodilatory effect is beneficial for asthmatic patients Versed and ativan are the most commonly encountered benzodiazepine sedatives, but they are infrequently used because they increase the risk of delirium and delay extubation Benzodiazepines are useful for sedation in patients with delirium tremens For post intubation analgesia, fentanyl is the drug of choice since it has a lower risk of hypotension than is seen in other narcotics In the emergency department, intubated and sedated patients should initially be sedated to a RASS of -2 while obtaining imaging, but aim for a RASS of -1 after to decrease side effects and promote earlier extubation References Ely EW, Truman B, Shintani A, et al. Monitoring sedation status over time in ICU patients: reliability and validity of the Richmond Agitation-Sedation Scale (RASS). JAMA. 2003;289(22):2983-2991. Garner O, Ramey JS, Hanania NA. Management of Life-Threatening Asthma: Severe Asthma Series. Chest. 2022. Keating GM. Dexmedetomidine: A Review of Its Use for Sedation in the Intensive Care Setting. Drugs. 2015;75(10):1119-1130. McKeage K, Perry CM. Propofol: a review of its use in intensive care sedation of adults. CNS Drugs. 2003;17(4):235-272. Ramos-Matos CF, Bistas KG, Lopez-Ojeda W. Fentanyl. In: StatPearls. Treasure Island (FL): StatPearls Publishing. Copyright © 2022, StatPearls Publishing LLC.; 2022. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD & Erik Verzemnieks, MD Emergency Medical Minute's Palliative screening event is tonight! There is still time to buy tickets to this intimate evening diving into the nuance of pediatric palliative care, purchase tickets on eventbrite!
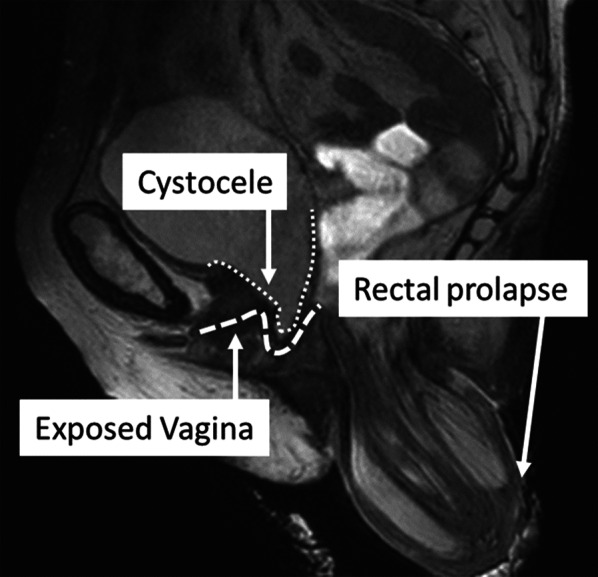
Podcast 792: Rectal Prolapse
Contributor: Jarod Scott, MD Educational Pearls: Rectal prolapse is an evagination of the rectal tissue through the anal opening Factors that weaken the pelvic floor muscles increase the risk of rectal prolapse These include age > 40, female, multiple pregnancies, constipation, diarrhea, cystic fibrosis, prior pelvic floor surgeries, or other pelvic floor abnormalities Noninvasive treatment options include increasing fluid and fiber intake to soften stools as well as using padding/taping to reinforce the perineum Surgery is an option to repair the prolapse so long as the patient is a good surgical candidate Medical sugar can be used as a desiccant to dry out and shrink the prolapse thus allowing for easier manual replacement References Coburn WM, 3rd, Russell MA, Hofstetter WL. Sucrose as an aid to manual reduction of incarcerated rectal prolapse. Ann Emerg Med. 1997;30(3):347-349. 2Gachabayov M, Bendl R, Flusberg M, et al. Rectal prolapse and pelvic descent. Curr Probl Surg. 2021;58(9):100952. Segal J, McKeown DG, Tavarez MM. Rectal Prolapse. In: StatPearls. Treasure Island (FL): StatPearls Publishing. Copyright © 2022, StatPearls Publishing LLC.; 202 Summarized by Mark O'Brien, MS4 | Edited by John Spartz MS4 & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 791: Hyperglycemic Hyperosmolar State
Contributor: Aaron Lessen, MD Educational Pearls: Hyperglycemic Hyperosmolar State (HHS) is less common than Diabetic Ketoacidosis (DKA) but is associated with a mortality rate up to 10 times greater than that seen in DKA Typically seen in elderly patients with severely elevated blood glucose levels (>1000 mg/dL) and an increased plasma osmolality Unlike in DKA, patients with HHS do not have elevated ketones Treatment of HHS includes insulin administration along with correcting fluid and electrolyte abnormalities When treating HHS, it is important to monitor and follow osmolality regularly because over-rapid correction can result in the development of cerebral edema References Fayfman M, Pasquel FJ, Umpierrez GE. Management of Hyperglycemic Crises: Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State. Med Clin North Am. 2017;101(3):587-606. Gosmanov AR, Gosmanova EO, Kitabchi AE. Hyperglycemic Crises: Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State. In: Feingold KR, Anawalt B, Boyce A, et al., eds. Endotext. South Dartmouth (MA): MDText.com, Inc. Copyright © 2000-2022, MDText.com, Inc.; 2000. Long B, Willis GC, Lentz S, Koyfman A, Gottlieb M. Diagnosis and Management of the Critically Ill Adult Patient with Hyperglycemic Hyperosmolar State. J Emerg Med. 2021;61(4):365-375. Summarized by Mark O'Brien, MS4 | Edited by John Spartz MS4 & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
On the Streets #14: Trauma Activations in the Field
The Emergency Medical Minute is excited to announce that we our upcoming event, Palliative. Check out our event page for more information and to buy tickets: Palliative Eventbrite Page
Podcast 790: Opioids vs OTC Pain Meds
Contributor: Aaron Lessen, MD Educational Pearls: NSAIDs are a potential alternative to opioids for pain management and are associated with decreased rates of adverse effects A recent study evaluated the effectiveness of ibuprofen and oxycodone for pain management in pediatric patients with isolated, acute-limb fractures Participants were discharged home with either ibuprofen or oxycodone and followed for six weeks There was no difference in pain scores between those taking ibuprofen and those taking oxycodone indicating that they had comparable analgesic effects Those in the ibuprofen group experienced significantly less adverse events compared to those taking oxycodone The participants in the ibuprofen group showed quicker return to their normal activities and improved quality of life In pediatric patients with fracture-related pain, ibuprofen is a safer alternative to oxycodone that is equally effective for pain control References Ali S, Manaloor R, Johnson DW, et al. An observational cohort study comparing ibuprofen and oxycodone in children with fractures. PLoS One. 2021;16(9):e0257021. Cooney MF. Pain Management in Children: NSAID Use in the Perioperative and Emergency Department Settings. Paediatr Drugs. 2021;23(4):361-372. Yin X, Wang X, He C. Comparative efficacy of therapeutics for traumatic musculoskeletal pain in the emergency setting: A network meta-analysis. Am J Emerg Med. 2021;46:424-429. Summarized by Mark O'Brien, MS4 | Edited by John Spartz MS4 & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we our upcoming event, Palliative. Check out our event page for more information and to buy tickets: Palliative Eventbrite Page Donate to EMM today!
Podcast 789: DOAC
Contributor: Aaron Lessen, MD Educational Pearls: Direct Oral Anticoagulants (DOACs) have surpassed Warfarin and Lovenox® for anticoagulation as they do not require injection and allow for easier discharge. In the ED, they are commonly prescribed after PE or DVT diagnosis. Common DOACs are Apixaban (Eliquis®) and Rivaroxaban (Xarelto®). There has not been a direct head to head study comparing outcomes. 2 large observational studies evaluated the recurrence of clots and bleeding risk in patients with newly prescribed Eliquis® or Xarelto® for DVT or PE. Both studies found that Eliquis® had superior outcomes. Further data is required to determine the preferred DOAC. A randomized trial comparing the two DOACs is upcoming with enrollment ending in 2023. References Dawwas GK, Leonard CE, Lewis JD, Cuker A. Risk for Recurrent Venous Thromboembolism and Bleeding With Apixaban Compared With Rivaroxaban: An Analysis of Real-World Data. Ann Intern Med. 2022;175(1):20-28. doi:10.7326/M21-0717 Aryal MR, Gosain R, Donato A, et al. Systematic review and meta-analysis of the efficacy and safety of apixaban compared to rivaroxaban in acute VTE in the real world. Blood Adv. 2019;3(15):2381-2387. doi:10.1182/bloodadvances.2019000572 Image from: Bristol-Myers Squibb Company. Eliquis 10 Million Patients and Counting. Sec.gov. https://www.sec.gov/Archives/edgar/data/14272/000114036119003478/s002621x16_425.htm. Accessed June 12, 2022. Summarized by Kirsten Hughes, MS4 | Edited by John Spartz MS4 & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Mental Health Monthly #13: Substance-Induced Psychosis (Part I)
Substance-Induced Psychosis (Part I) In this first episode of a two-part mini-series, we feature Dr. Nadia Haddad, a Colorado psychiatrist, and Dr. Ricky Dhaliwal, an emergency medicine physician, as they discuss the different substances that cause psychosis and their unique presentations in the ED and in the psychiatric world. First, Dr. Haddad establishes a medical definition of psychosis. Then, Dr. Haddad and Dr. Dhaliwal partake in a fruitful discussion, each providing their unique perspective on the drugs that affect our patient populations today. Key Points: Psychosis is a cognitive processing disorder, which leads to auditory hallucinations, visual hallucinations, and delusions. Axis one psychosis like that from schizophrenia or mania typically produces auditory hallucinations, not visual hallucinations. Delusions are also common in underlying psychiatric psychosis. One of the most common substances that cause psychosis today is methamphetamine. Meth-induced psychosis can mimic schizophrenia symptoms, though tactile hallucinations are very common with methamphetamine use. Methamphetamine is active for up to about 8 hours but can vary depending on underlying mental health predispositions, which can be exacerbated for several days or a week before neurotransmitters right themselves after meth use. Cannabis can lead to psychosis and paranoia for people - especially young people - with a predisposition to schizophrenia or bipolar. Alcohol-related psychosis comes primarily from withdrawal, though acute alcohol intoxication may cause mild alcoholic hallucinosis. The hallmark of delirium tremens is a fluctuating, waxing-and-waning consciousness, which can occur 72 hours after the last drink. DTs can occur after treatment of the physical withdrawal symptoms. Alcohol withdrawal can occur even at high BALs relative to a patient's baseline. Cocaine psychosis is similar to methamphetamine-induced psychosis. Recorded, Summarized, and Edited By: Jorge Chalit

Podcast 788: Tracheostomy Bleeding
Contributor: Aaron Lessen, MD Educational Pearls: Tracheostomy bleeding is a rare but potentially life-threatening complication that usually occurs within the first month of tracheostomy tube placement No matter how severe the bleeding, every patient should be evaluated to rule out a tracheo-innominate fistula between the tracheostomy and the innominate artery If the patient is currently bleeding and has a cuffed tracheostomy tube, over-inflate the balloon to compress the bleeding vessel Consider replacing an uncuffed tracheostomy tube with a cuffed tube or an ET tube If the tracheostomy was performed in the last seven days, use a bougie or bronchoscope to replace the uncuffed tube due to increased risk of opening a false track into the subcutaneous tissue If bleeding cannot be controlled, follow mass-transfusion protocols, and as a last resort, remove the tube and insert a finger into the stoma to manually compress the artery References Bontempo LJ, Manning SL. Tracheostomy Emergencies. Emerg Med Clin North Am. 2019;37(1):109-119. Khanafer A, Hellstern V, Meißner H, et al. Tracheoinnominate fistula: acute bleeding and hypovolemic shock due to a trachea-innominate artery fistula after long-term tracheostomy, treated with a stent-graft. CVIR Endovasc. 2021;4(1):30. Manning Sara, Bontempo Laura. Complications of Tracheostomies. In: Mattu A and Swadron S, ed. ComPendium. Burbank, CA: CorePendium, LLC. https://www.emrap.org/corependium/chapter/reckOdDn9Ljn7sBLy/Complications-of-Tracheostomies. Updated August 17, 2021. Accessed June 5, 2022. Summarized by Mark O'Brien, MS4 | Edited by John Spartz, MD, MPH & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 787: TAVR and Stroke
Contributor: Nick Hatch, MD Educational Pearls: Transcatheter aortic valve replacement (TAVR) is an increasingly common endovascular procedure to treat aortic stenosis TAVR is an alternative to the open approach surgical aortic valve replacement (SAVR) for patients who are inoperable or are high risk surgical candidates Following TAVR, there is increased risk of stroke, particularly in the first 30 days TAVR-related strokes are due to embolic debris left on the valve root, which is generally cleaned out during SAVR Further, following the procedure many patients are anticoagulated which increases the risk for conversion to hemorrhagic stroke Isolated, unexplained nausea and vomiting in elderly patients should prompt concern for a neurologic workup with imaging - even more so if they have recently undergone TAVR References Davlouros PA, Mplani VC, Koniari I, Tsigkas G, Hahalis G. Transcatheter aortic valve replacement and stroke: a comprehensive review. J Geriatr Cardiol. 2018;15(1):95-104. doi:10.11909/j.issn.1671-5411.2018.01.008 Gleason TG, Reardon MJ, Popma JJ, et al. 5-Year Outcomes of Self-Expanding Transcatheter Versus Surgical Aortic Valve Replacement in High-Risk Patients. J Am Coll Cardiol. 2018;72(22):2687-2696. doi:10.1016/j.jacc.2018.08.2146 Siontis GCM, Overtchouk P, Cahill TJ, et al. Transcatheter aortic valve implantation vs. surgical aortic valve replacement for treatment of symptomatic severe aortic stenosis: an updated meta-analysis. Eur Heart J. 2019;40(38):3143-3153. doi:10.1093/eurheartj/ehz275 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz MS4 & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!

Podcast 786: Smiling Death
Contributor: Nick Hatch, MD Educational Pearls: "Smiling Death" describes the prehospital phenomenon of a person who is happy to be extricated from an extended period of crush injury, but dies suddenly soon after the rescue. Smiling Death is caused by Crush Syndrome. Crush Syndrome begins when large areas of tissue are damaged by compression and subsequent impeded blood flow. Resultant cell death is followed by release of myoglobin and efflux of electrolytes including potassium. Upon removal of the crushing force, high levels of potassium enter circulation and cause cardiac arrhythmias leading to sudden death. Prevention measures include aggressive hydration using normal saline before extrication. An acceptable starting rate is 1L per hour, but providers should take patient status into consideration and titrate appropriately. Standard techniques for controlling hyperkalemia by intracellular shifting may be less effective. Early dialysis may be useful. References Gonzalez D. Crush syndrome. Crit Care Med. 2005;33(1 Suppl):S34-S41. doi:10.1097/01.ccm.0000151065.13564.6f Better OS. Rescue and salvage of casualties suffering from the crush syndrome after mass disasters. Mil Med. 1999;164(5):366-369. Summarized by Kirsten Hughes, MS4 | Edited by John Spartz MS4 & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!

Podcast 785: Pepper Spray
Contributor: Jared Scott, MD Educational Pearls: Pepper spray is a chemical irritant derived from oleoresin capsicum (OC), an extract from pepper plants. It can be used by police for riot or crowd control, or by individuals for self defense. In the event of an exposure, those affected should immediately disperse from the area, remove contact lenses with clean or gloved hands, and remove contaminated clothing. Pepper spray can spread from patients to providers by contact. When caring for those exposed, providers should use PPE including gloves and should double bag personal belongings. For patient management consider the following: If the eyes are affected, first remove contacts then irrigate with clean water. Use proparacaine drops for relief. Clean exposed skin thoroughly with soap and water. Inhalation and ingestion may cause nausea, vomiting, shortness of breath and generalized anxiety from discomfort. Treatment can include antiemetics and anxiolytics. Symptoms may persist for many days. References Schep LJ, Slaughter RJ, McBride DI. Riot control agents: the tear gases CN, CS and OC-a medical review. J R Army Med Corps. 2015;161(2):94-99. doi:10.1136/jramc-2013-000165 Tidwell RD, Wills BK. Tear Gas and Pepper Spray Toxicity. [Updated 2022 Jan 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544263/ Summarized by Kirsten Hughes, MS4 | Edited by John Spartz MS4 & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today! *********************

Podcast 784: Wastewater Surveillance for COVID
Contributor: Jared Scott, MD Educational Pearls: About 50% of those infected with SARS-CoV-2 will shed the virus in their feces Wastewater surveillance can be used to track COVID burden, which may be easier than collating test data from multiple hospitals across a region Viral shedding begins 5-7 days prior to symptom onset, so wastewater data can be used to anticipate outbreaks and inform policy and public health initiatives Some existing limitations to wastewater surveillance include: Reporting by counties were water sources may be mixed Septic tanks and other closed water systems will not be counted Not all those infected will shed the virus References Weidhaas J, Aanderud ZT, Roper DK, et al. Correlation of SARS-CoV-2 RNA in wastewater with COVID-19 disease burden in sewersheds. Sci Total Environ. 2021;775:145790. doi:10.1016/j.scitotenv.2021.145790 Kirby AE, Walters MS, Jennings WC, et al. Using Wastewater Surveillance Data to Support the COVID-19 Response — United States, 2020–2021. MMWR Morb Mortal Wkly Rep 2021;70:1242–1244. DOI: http://dx.doi.org/10.15585/mmwr.mm7036a2 Covid-19 monitoring in wastewater. Colorado COVID-19 Updates. https://covid19.colorado.gov/covid-19-monitoring-in-wastewater. Accessed May 21, 2022. Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD, MPH & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!
Podcast 783: LAD Occlusion & Troponin
Contributor: Jared Scott, MD Educational Pearls: A study randomized 34 healthy patient to have their left anterior descending artery (LAD) occluded by balloon for 0, 15, 30, or 90 seconds Subsequently, cardiac troponins (cTns) and Copeptin were measured every 15 minutes for 3 hours, then every 30 minutes for the next 3 hours 5 conclusions were drawn: Copeptin is not a useful marker of cardiac ischemia cTn may be detected after only 30 seconds of ischemia cTn may be detected in a little as 15 minutes after ischemic event After only 90 seconds of ischemia, cTn levels met threshold for MI Troponin I is a better marker than troponin T as it rises faster and reaches a higher peak Patients very recent or very brief ischemic events may have elevated troponin in the ED References Árnadóttir Á, Pedersen S, Bo Hasselbalch R, et al. Temporal Release of High-Sensitivity Cardiac Troponin T and I and Copeptin After Brief Induced Coronary Artery Balloon Occlusion in Humans [published correction appears in Circulation. 2021 Jun 22;143(25):e1116]. Circulation. 2021;143(11):1095-1104. doi:10.1161/CIRCULATIONAHA.120.046574 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz, MD, MPH & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!

Podcast 782: Ventilator Management
Contributor: Aaron Lessen, MD Educational Pearls: Tidal volume is the amount of breath a patient receives in a single ventilation Traditional tidal volume (TV) setting was 10 ml/kg but studies showed lower TV had less incidence of respiratory distress, ARDS, and overall better outcomes ED ventilation settings may get carried on for hours or days when a patient is admitted, making this an important part of patient care Recent large systematic review shows that low TV setting in the ED leads to decreased incidence of ARDS, shorter ICU and hospital length of stay, shorter duration of mechanical ventilation, and decreased mortality Consider an ED low tidal volume ventilation setting at around 6 ml/kg of predicted body weight References De Monnin K, Terian E, Yaegar LH, et al. Low Tidal Volume Ventilation for Emergency Department Patients: A Systematic Review and Meta-Analysis on Practice Patterns and Clinical Impact [published online ahead of print, 2022 Feb 7]. Crit Care Med. 2022;10.1097/CCM.0000000000005459. doi:10.1097/CCM.0000000000005459 Summarized by Kirsten Hughes, MS4 | Edited by John Spartz MS4 & Erik Verzemnieks, MD The Emergency Medical Minute is excited to announce that we are now offering AMA PRA Category 1 credits™ via online course modules. To access these and for more information, visit our website at https://emergencymedicalminute.org/cme-courses/ and create an account. Donate to EMM today!