Emergency Medical Minute
1,164 episodes — Page 19 of 24
Podcast #249: D-Dimer
Author: Michael Hunt, M.D. Educational Pearls In the recent YEARS study, investigators checked every patient with suspicion for PE with a D-dimer, using a modified Wells score for risk stratification. The goal of the study was to show that CT scan usage could safely reduced using this screening method. The Wells Criteria measures they used to stratify risk were: PE mostly likely dx, hemoptysis, and evidence of DVT. If the d-dimer was 1, but the patient had none of the Wells criteria, the patient did not get a CT. If the patient had any of the criteria, but the d-dimer was only 0.5, the patient did not get a CT scan. The investigators reduced CT usage by 14% using the new criteria, with no significant increase in morbidity and mortality. References: van der Hulle et al. Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): a prospective, multicentre, cohort study. The Lancet. 2017
Podcast #248: Patent Foramen Ovale
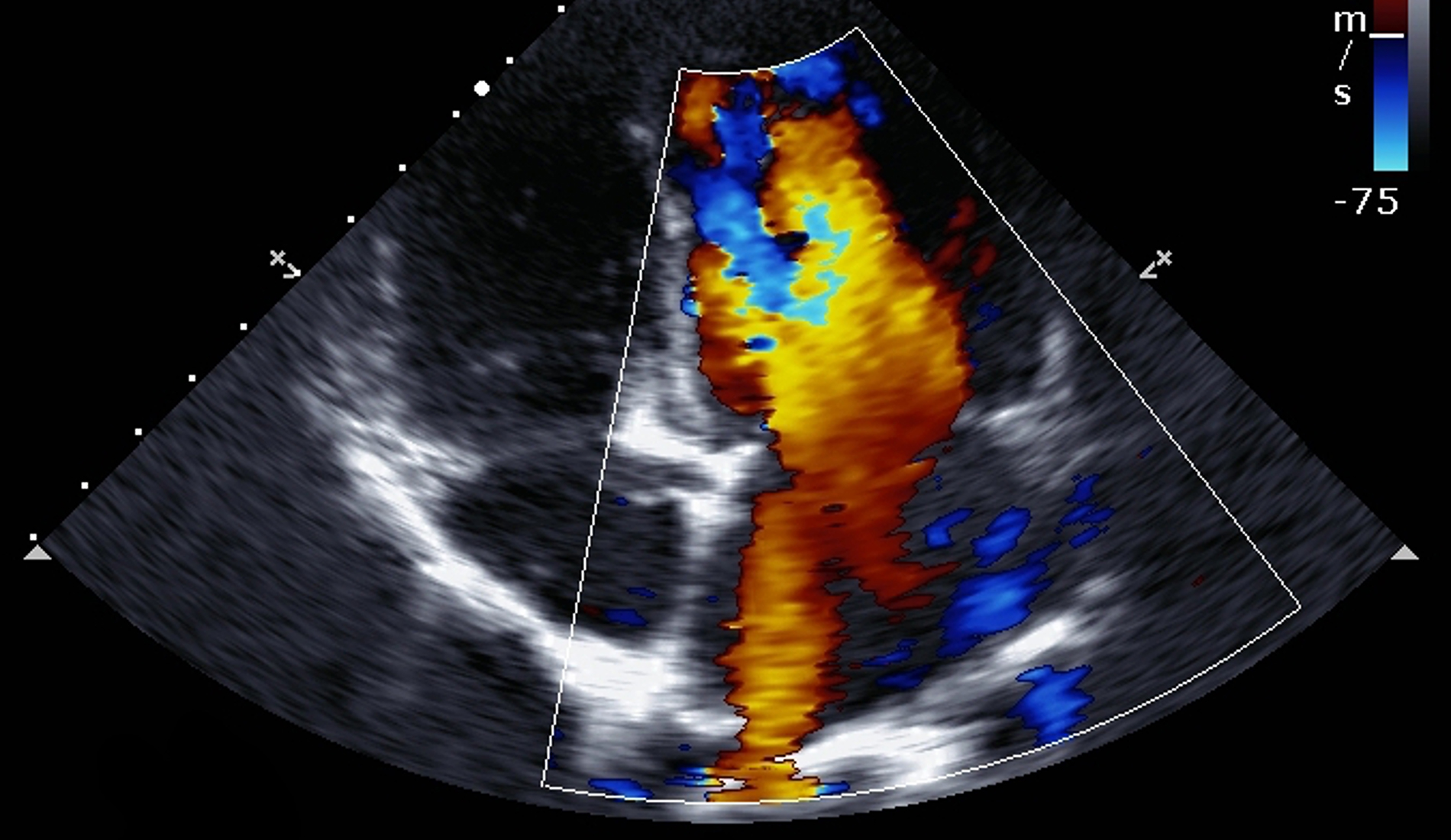
Author: Jared Scott, M.D. Educational Pearls The foramen ovale (FO) connects the left and right atria to allow oxygenated blood to bypass the developing lungs, it usually closes at birth but for some it remains patent (PFO). A PFO allows clots to cross from the venous to arterial circulation, increasing the likelihood of stroke. PFO is present in 25% of general population, present in 50% of those with stroke of unknown cause, and very common those with stroke under 50 years old. Treat with anticoagulation or surgical correction. References: http://www.heart.org/HEARTORG/Conditions/More/CardiovascularConditionsofChildhood/Patent-Foramen-Ovale-PFO_UCM_469590_Article.jsp#.WarsZZN95E4

Podcast #247: Are You Listening? - 3 Ear Emergencies You Can't Miss!
Author: Don Stader, M.D. Educational Pearls Ear pain is a common complaint in adults and kids. A red, hot, painful ear with involvement of the pinna could indicate perichondritis - an infection of the cartilage that is usually caused by pseudomonas. A painful, swollen ear with involvement of the mastoid process could be mastoiditis, which needs to be treated with IV antibiotics to avoid cerebellar abscess. Ear pain with significant drainage and a cranial nerve deficit points to malignant otitis externa, which needs to be treated with IV antibiotics. References: John W. Ely, Marlan R. Hansen, Elizabeth C. Clark. Diagnosis Of Ear Pain. 2008. American Family Physician.

Podcast #246: Fever in Sepsis
Author: Nick Hatch, M.D. Educational Pearls A recent observational cohort study found that the biggest predictor for sepsis survival was fever. Those with higher fevers had better outcomes. Some possible explanations for this finding are that high fevers indicate good immune response or that high fever cued providers to treat sepsis more aggressively. References: Paul J Young, Rinaldo Bellomo. Fever in Sepsis: is it cool to be hot?. 2014. Critical Care

Podcast #245: Hypoglycemia
Author: Dylan Luyten, M.D. Educational Pearls Hypoglycemia is very common in type 2 diabetics, and is often caused by insulin overdose or missed meals. Knowing the peak time of action for common diabetes medications can help inform treatment and disposition. Regular insulin's action peaks around 60 minutes. By the time most of these patients present to the ED, the drug has had most of its effect. Lantis' action does not peak, and will continue to exert its effect for 12 or more hours. Levamir has a peak around 6-8 hours. Metformin sensitizes tissues to insulin, so it cannot cause hypoglycemia alone. Glipizides have half-lives over 12 hours and work by increasing insulin release by the pancreas. Hypoglycemia in a patient taking a glipizide usually indicates there is another medical issue interfering with clearance References: http://emedicine.medscape.com/article/122122-workup
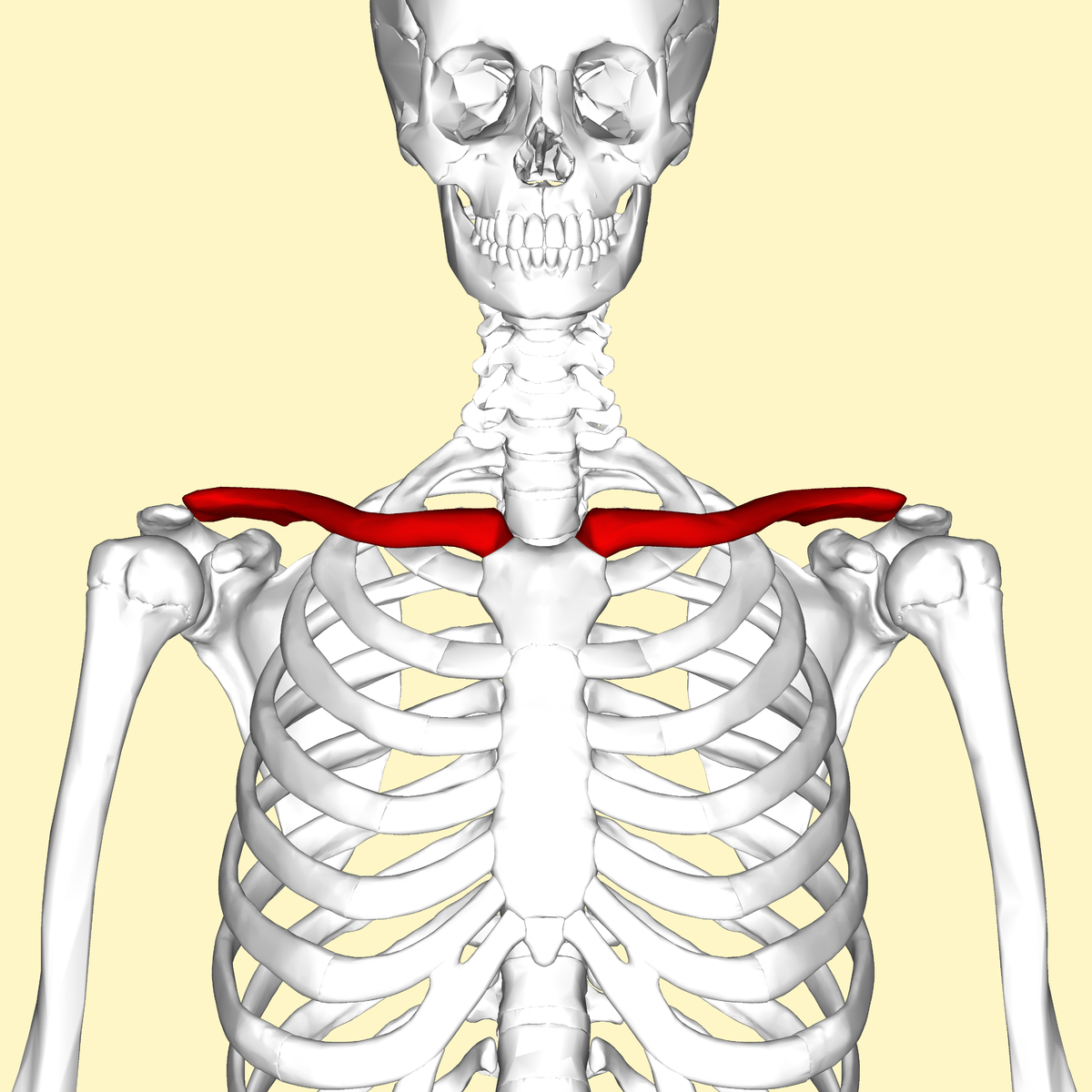
Podcast #244: Clavicle Fracture Review
Author: Nick Hatch, M.D. Educational Pearls The force required to break a clavicle is significant, so clavicle fracture may be associated with other injury (pneumothorax, vascular injury). Most fractures occur in the middle 1/3 of the clavicle. Traditionally, clavicle fractures have been managed without surgery. However, recent studies have shown that surgery may be beneficial in a larger population than previously thought. References: http://emedicine.medscape.com/article/398799-overview

Podcast #243: Sphenopalatine Nerve Block
Author: Don Stader, M.D. Educational Pearls Cluster headaches are usually intense, unilateral, and involve the periorbital area. CN V (Trigeminal) provides sensory and autonomic innervation the face and eyes, which play roles in headache pathology. Cluster headaches can be treated with high flow oxygen, but a new treatment involves blocking the sphenopalatine ganglion (SPG) with lidocaine. Because sensory and autonomic branches of the trigeminal traverse the SPG, lidocaine will effectively treat a cluster headache. To block the ganglion, intranasal lidocaine may be used, or a Q-tip soaked in 4% lidocaine can be applied to the most posterior aspect of the pharynx for 10-15 minutes. References: https://www.aliem.com/2017/03/trick-sphenopalatine-ganglion-block-primary-headaches/
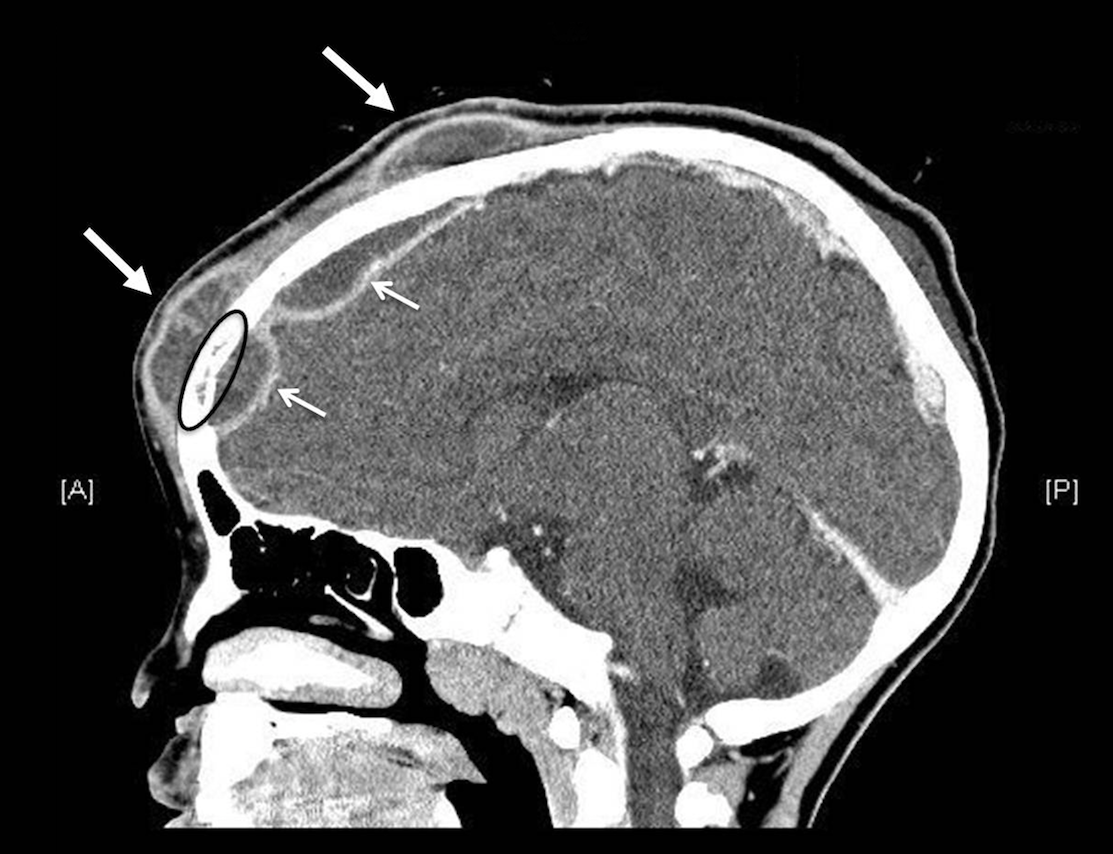
Podcast #242: Pott's Puffy Tumor
Author: Suzanne Chilton, M.D. Educational Pearls Pott's puffy tumor is a subperiosteal abscess of the frontal bone that arises from hematologic spread or direct infection via the frontal sinuses. The primary symptom is facial swelling. It is much more common in children and adolescents. Treatment involves removal of the frontal bone, reconstructive surgery, and 6-8 weeks of IV antibiotics. References: Grewal HS, Dangaych NS, Esposito A. A tumor that is not a tumor but it sure can kill! The American Journal of Case Reports. 2012;13:133-136. doi:10.12659/AJCR.883236.

Podcast #241: GERD vs. MI
Author: Dave Rosenberg, M.D. Educational Pearls MI and GERD can present similarly. For example, 47% with angina report increased belching with an anginal attack, and 20% of people with an MI describe symptoms of indigestion that are relieved by antacids. Overall, GERD is more common in those with CAD, so don't be "reassured" by GERD symptoms in the setting of chest pain. References: http://www.mdedge.com/ecardiologynews/article/82215/cad-atherosclerosis/gerd-may-boost-risk-mi

Podcast #240: Honey and Burns
Podcast #240: Honey and Burns Author: Nick Hatch, M.D. Educational Pearls Honey can be used to treat burns because it has antibacterial properties. In one study, honey outperformed silver sulfadiazine for burn treatment, but more research is needed in this area. In practice, honey is likely more useful outside the ER than inside the ER. References: Gupta SS, Singh O, Bhagel PS, Moses S, Shukla S, Mathur RK. Honey Dressing Versus Silver Sulfadiazene Dressing for Wound Healing in Burn Patients: A Retrospective Study. Journal of Cutaneous and Aesthetic Surgery. 2011;4(3):183-187. doi:10.4103/0974-2077.91249.

Podcast #239: Tetanus in the ED
Author: Rachel Beham, PharmD, Advanced Clinical Pharmacist - Emergency Medicine Educational Pearls Tetanus Ig is indicated in those who have no or unknown tetanus vaccination history who present with contaminated cuts that or dirty puncture wounds The tetanus vaccine is a 5 shot series (DTAP) for children, TDAP is used for adults There is no harm is receiving the TDAP more than once if vaccination history is unknown References: https://www.cdc.gov/features/tetanus/index.html
Podcast #238: Ultrasound in Cardiac Arrest
Author: Aaron Lessen M.D. Educational Pearls Ultrasound is helpful in the setting of cardiac arrest for finding a cause like cardiac tamponade or PE, but also for predicting outcomes for non-shockable rhythms. One study showed that in those that presented with asystole or PEA and cardiac activity on US had a 4% survival rate, while those without cardiac activity had almost no chance. References: Philip Salen, Larry Melniker, Carolyn Chooljian, John S. Rose, Janet Alteveer, James Reed, Michael Heller, Does the presence or absence of sonographically identified cardiac activity predict resuscitation outcomes of cardiac arrest patients?, The American Journal of Emergency Medicine, Volume 23, Issue 4, 2005, Pages 459-462, ISSN 0735-6757, http://dx.doi.org/10.1016/j.ajem.2004.11.007.

Deep Dive #5: The Evolution of Sepsis Treatment
Author: Susan Brion, M.D. Dr. Brion enlightens us on the ever-evolving standard of sepsis management.

Podcast #237: Phimosis vs. Paraphimosis
Author: Sam Killian, M.D. Educational Pearls Phimosis refers to the inability to retract the distal foreskin over the glans penis in uncircumcised males. Paraphimosis is the entrapment of the foreskin proximal to the glans penis in these patients. Phimosis is rarely a medical emergency, but requires follow up with urology. Paraphimosis, on the other hand, can cause venous and lymphatic insufficiency, leading to infarction, necrosis and autoamputation. Therefore, paraphimosis requires emergent treatment with manual reduction of the foreskin or surgery. References: Aaron Vunda, M.D., Laurence E. Lacroix, M.D., Franck Schneider, Sergio Manzano, M.D., and Alain Gervaix, M.D. Reduction of Paraphimosis in Boys. N Engl J Med 2013; 368:e16

Podcast #236: Peripheral IJ Access
Author: Nick Hatch, M.D. Educational Pearls When peripheral or central IV access is difficult, sometimes providers will try to use a peripheral IV setup at an IJ site using US guidance. Case studies have shown that this method is often successful, with the most common complication being the loss of access. References: Ash AJ, Raio C. Seldinger Technique for Placement of "Peripheral" Internal Jugular Line: Novel Approach for Emergent Vascular Access. Western Journal of Emergency Medicine. 2016;17(1):81-83. doi:10.5811/westjem.2015.11.28726.

Podcast #235: ER Discharge and Mortality
Author: Pete Bakes, M.D. Educational Pearls One of the roles of the ER provider is to discharge patients only after life-threatening conditions have been ruled out. However, some patients that are discharged from the ED die within days of their discharge. One recent study sought to investigate the factors and diagnoses associated with death within 7 days of discharge. This study was a retrospective study in 10 million medicare recipients that presented to the ER over 10 years. They excluded palliative, hospice and SNF patients. 0.12% of these patients died within 7 days of ER discharge. Signs and symptoms such as altered mental status, general malaise and fatigue, and nonspecific dyspnea had relative risks of 3-5 for death following discharge. Think carefully before discharge in patients with the signs/symptoms above. References: Obermeyer Ziad, Cohn Brent, Wilson Michael, JenaAnupam B, Cutler David M. Early death after discharge from emergency departments: analysis of national US insurance claims data BMJ 2017;356 :j239

Podcast #234: CIN AEM Study
Author: Dylan Luyten, M.D. Educational Pearls Around 30% of patients in the ER receive CT imaging, and the sensitivity of CT imaging may be improved with IV contrast. However, contrast is often withheld for fear of contrast-induced nephropathy. A recent, single-center, retrospective cohort study compared the rates of nephropathy between contrast CT, non-contrast CT, and no CT control patients, and found no differences. This study confirms what many have believed to be true - that the dangers of modern contrast may be overstated. However, the results should be interpreted with caution, as this was a retrospective, single-center study. References: Hinson, Jeremiah S. et al.. Risk of Acute Kidney Injury After Intravenous Contrast Media Administration. Annals of Emergency Medicine , Volume 69 , Issue 5 , 577 - 586.e4

Podcast #233: Carfentanil
Author: Don Stader, M.D. and Rachael Duncan, PharmD BCPS BCCCP Educational Pearls Carfentanil is an opioid elephant tranquilizer that can be used recreationally. It is 1000 times stronger than fentanyl, and looks like a white powder. Healthcare workers must be cautious when carfentanil overdose is suspected, as the drug can be absorbed through caregivers' skin if it is present on the patient's clothes. Overdose may require large amounts of naloxone, and a drip may be started at a rate equivalent to the bolus dose that the patient responded to. For example, if the patient responded to a 10mg bolus dose of naloxone, he would then be started on a 10mg/hr naloxone drip. References: https://www.dea.gov/divisions/hq/2016/hq092216.shtml

Podcast #232: HAPE
Author: Gretchen Hinson, M.D. Educational Pearls High-Altitude Pulmonary Edema (HAPE) is caused when hypoxemia due to low ambient pO2 leads to breakdown and constriction of the pulmonary vasculature leading to edema. HAPE is very rare under 8000 ft, but common over 10000 ft (6%). Over 18,000 ft the incidence is very high (12-15%). Symptoms include dyspnea, cough, weakness and chest tightness. Signs include hypoxemia, crackles, wheezing, central cyanosis, tachypnea and tachycardia. Drugs that reduce pulmonary resistance have been shown to help, but increased oxygenation and descent are the best treatments. References: http://emedicine.medscape.com/article/300716-overview
Podcast #231: Esophageal Tearing
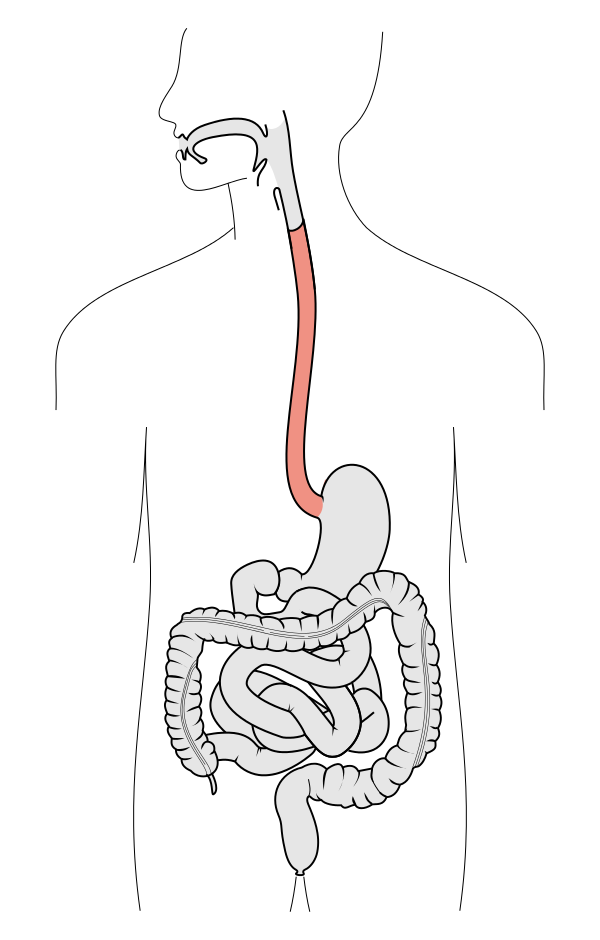
Author: Jared Scott, M.D. Educational Pearls Boerhaave syndrome (aka effort rupture of the esophagus) accounts for 10% of esophageal ruptures and is usually caused by strain during vomiting episodes. It can also be caused by childbirth, seizure, or prolonged coughing or laughing. Food and water swallowed after the tear end up in the mediastinum, eventually causing infection. Therefore, Boerhaave syndrome is a surgical emergency. Best diagnostic techniques are CT or endoscopy. Mallory-Weiss syndrome may present similarly, however it is less serious since it involves only a small tear through the mucosa at the gastroesophageal junction. This can be managed on an outpatient basis with PPI's. References: https://radiopaedia.org/articles/boerhaave-syndrome

Podcast #230: Concussive Treatment
Author: Aaron Lessen, M.D. Educational Pearls 2 studies this past year looked at pediatric and adolescent patients following a concussion. They found people who returned to activity sooner did better than those who went on "brain rest". While patients should still follow up with their PCP following a concussion, it is ok for patients to return to physical activity as tolerated. References: Grool AM, Aglipay M, Momoli F, Meehan WP, Freedman SB, Yeates KO, Gravel J, Gagnon I, Boutis K, Meeuwisse W, Barrowman N, Ledoux A, Osmond MH, Zemek R, for the Pediatric Emergency Research Canada (PERC) Concussion Team. Association Between Early Participation in Physical Activity Following Acute Concussion and Persistent Postconcussive Symptoms in Children and Adolescents. JAMA. 2016;316(23):2504-2514. doi:10.1001/jama.2016.17396
Podcast #229: Andrew Jackson
Author: Sam Killian, M.D. Educational Pearls Andrew Jackson was the 7th president of the USA. He served 2 terms from 1829-1837. He had had many medical issues during his presidency. He was said to be chronically underweight with rotting teeth. Furthermore, he had chronic infections and lead poisoning from bullets lodged in his arm and chest. He suffered from smallpox that he contracted while in a British prison during the Revolutionary War. He died from "dropsy" (CHF). References: http://www.doctorzebra.com/prez/g07.htm

Podcast #228: BB Guns
Author: Jared Scott, M.D. Educational Pearls BB gun eye injuries are most common in August and September. They most often happen to males aged 16-17 year old. Around 10% of the BB eye injuries lead to eye loss. Accidental firearm injury is common in children and is a common cause of mortality. One-third of homes with children have a firearm. Most accidental pediatric gun injuries happen to young, male children with guns owned by family members. It is important to educate gun owners about proper gun storage. References: Childhood Firearm Injuries in the United States Katherine A. Fowler, Linda L. Dahlberg, Tadesse Haileyesus, Carmen Gutierrez, Sarah Bacon. Pediatrics Jun 2017, e20163486; DOI: 10.1542/peds.2016-3486

Podcast #227: CPR-Induced Consciousness
Author: Nick Hatch, M.D. Educational Pearls CPR-induced consciousness is a phenomenon that occurs when someone who was previously unconscious and is undergoing CPR regains consciousness and makes purposeful movements. Studies have shown that this phenomenon is increasing, likely because of increased quality of CPR. Many people use a sedative such as ketamine to keep patients unconscious to reduce the psychologic trauma of CPR. 39% of people who survive CPR with good neurologic details remember the process of CPR . References: Joshua Pound, P. Richard Verbeek, and Sheldon Cheske. CPR Induced Consciousness During Out-of-Hospital Cardiac Arrest: A Case Report on an Emerging Phenomenon. 2017. Prehospital Emergency Care Vol. 21.
Podcast #226: Biphasic Anaphylaxis
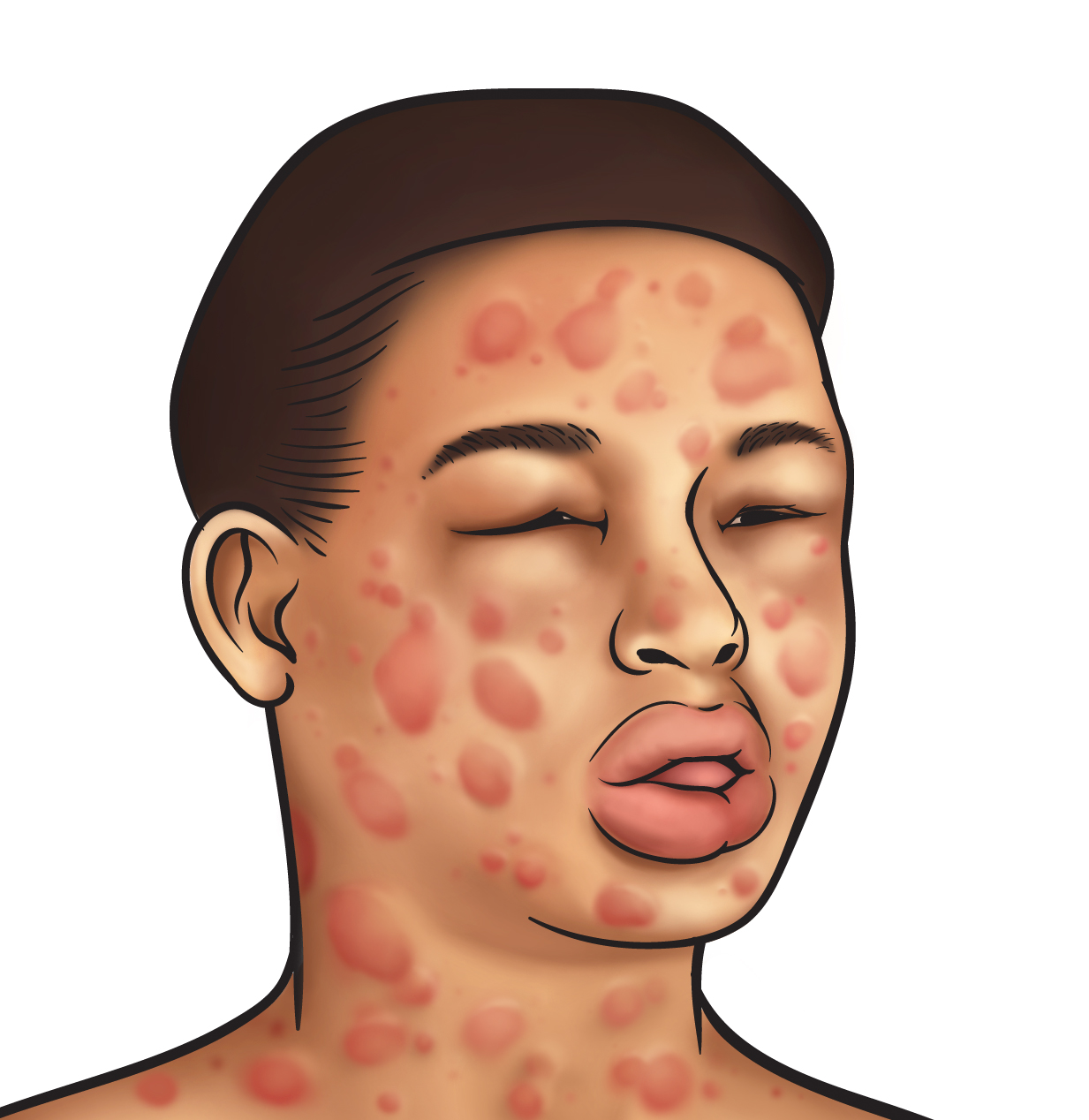
Author: Sam Killian, M.D. Educational Pearls Anaphylaxis is common in the ED. These patients are treated and then usually watched for 4-6 hours. Biphasic happens in patients that have a complete resolution of their anaphylaxis for at least an hour, but then have a recurrence that requires pharmacologic intervention. Most of the time this happens 3-6 hours later, but can happen more than 10 hours later. More commonly happens in patients that have a delayed presentation, a wide pulse pressure, need multiple doses of epi, require the use of a beta agonist, or are ages 6-9 years old. Educate patients about the possibility of Biphasic anaphylaxis before discharge. References: http://www.medscape.org/viewarticle/583328_7

Podcast #225: Rhogam
Author: Dylan Luyten, M.D. Educational Pearls Rhogam is commonly used when an Rh negative woman has an Rh positive fetus. It is commonly used in the ER in the setting of a miscarriage. Rh(+) fetal blood can enter the Rh(-) maternal circulation, sensitizing the woman to the Rh antigen. During a subsequent pregnancy, if the fetus is Rh(+), the woman may mount an immune response to the fetus, lead to fetal demise. Rhogam is used to block this process. Use of Rhogam has reduced this complication from 16% of Rh(+) pregnancies in the 1960's to less than 1% today. Under 10 weeks, the amount of maternal-fetal blood exchange is very small, so the use of Rhogam in a 1st trimester miscarriage is unnecessary. It should be used in patients with a miscarriage after 12 weeks, or women undergoing a surgical D&C. Rhogam is expensive and in limited supply, so it is important to only use it when necessary. References: Hannafin, Blaine et al. Do Rh-negative women with first trimester spontaneous abortions need Rh immune globulin? 2006. The American Journal of Emergency Medicine, Volume 24 , Issue 4 , 487 - 489

Deep Dive #4: Pediatric Type I DKA
Author: Justin Harper Justin Harper, a paramedic married to a pediatric nurse, discovered his own son had type I diabetes 2 years ago. Despite their medical experience, this diagnosis came as surprise to Justin and his wife. This is the compelling story about how their son was diagnosed with type I diabetes and how this has impacted their lives.

Brewcast Part VIII: Cannabis in Colorado
Author: Dr. Larry Wolk, Executive Director and Chief Medical Officer for the Colorado Department of Public Health and Environment. Topic: Dr. Larry Wolk educates us on how cannabis has affected Colorado since medical and recreational legalization.

Brewcast Part VII: A Patient's Perspective on Medical Marijuana
Authors: Don Stader, M.D. & Lauren Gibbs Topic: Lauren breaks the stoner stereotype and explains how marijuana has positively impacted her life.

Brewcast Part VI: Synthetic Marijuana
EAuthor: Erik Verzemnieks, M.D. Topic: Erik speaks about how slightly altering the chemical composition of marijuana can create a drug with drastic effects on the human body. WARNING: Explicit Language

Brewcast Part V: Researching Cannabis
Author: Sophie Yorkwilliams -B.A. (Psychology) -Dual Ph.D. Candidate, Clinical Psychology and Neuroscience. Expected graduation: 2020 Topic: Studying cannabis comes with its own set of challenges. Find out how Sophie and her team have overcome obstacles to get accurate data on marijuana.

Brewcast Part IV: A Physician's Perspective on Medical Marijuana
Authors: Don Stader, M.D. & Peter Pryor, M.D. Topic: What caused Dr. Pryor to leave emergency medicine and enter the realm of medical marijuana?

Brewcast Part III: Cannabinoid Hyperemesis Syndrome
Author: Rachael Duncan, PharmD BCPS BCCCP Topic: Rachel explains the science behind one of the most common maladies thought to be induced by chronic cannabis use.

Brewcast Part II: Pharmacology of Cannabis
Author: Brett Marlin, M.D. Topics: Brett explains the biochemical and physiological properties of cannabis.
Brewcast Part I: The History of Cannabis in Medicine
Author: Don Stader, M.D Topic: Don kicks things off with an overview of the history of marijuana and how it has made its way into medicine.
Podcast #224: Troponin
Author: Sam Killian, M.D. Educational Pearls Not every troponin elevation is an MI. Trop elevates in about an hour in ACS and stays elevated for days. Non-MI conditions that cause elevated troponin: Critical illness (sepsis), increased cardiac demand, right heart strain, LV dysfunction, hypotension, pressor use, acute PE, SAH, chronic renal failure, CHF, aortic dissection, and peri/myocarditis. Elevated troponin in settings other than MI is correlated with increased mortality. References: Korff S, Katus HA, Giannitsis E. Differential diagnosis of elevated troponins. Heart. 2006;92(7):987-993. doi:10.1136/hrt.2005.071282.

Podcast #223: Acyclovir Toxicity
Author: Nick Hatch, M.D. Educational Pearls Acyclovir toxicity can uncommonly cause altered mental status, low blood glucose, hallucinations and myoclonic jerks. Toxicity often occurs in the setting of renal insufficiency, as it is cleared by the kidneys. Acyclovir is often used to treat shingles, which can also cause similar symptoms as acyclovir toxicity due to encephalitis - rule this out in the setting of a concomitant shingles infection. References: http://www.rxlist.com/zovirax-drug.htm

Podcast #222: Wells Criteria for PE
Author: Michael Hunt, M.D. Educational Pearls Wells Criteria was initially designed to screen patients for further workup for PE. Aspects of the Wells Criteria include: signs and symptoms of DVT (3 points), PE most likely dia (3 points), HR > 100 (1.5 points), immobility for > 3 days or surgery in last 4 weeks (1.5 points), documented history of PE (1.5), hemoptysis (1), treatment for cancer in last 6 mo (1). ACEP uses a score of less than or equal to 4 to define "low risk." Greater than 4 is "high risk". Use Wells to guide clinical decisions about PE workup. References: http://www.ebmedicine.net/media_library/files/1212%20Pulmonary%20Embolism

Podcast #221: Walking Corpse Syndrome
Podcast #221: Walking Corpse Syndrome Author: Erik Verzemnieks, M.D. Educational Pearls Walking Corpse Syndrome (aka Cotard Delusion) is a very rare psychiatric disorder that leads to the belief that one is a "walking corpse". Often co-presents with depression, schizophrenia, and starvation. Responds to ECT. References: https://en.wikipedia.org/wiki/Cotard_delusion

Podcast #220: A-Fib Cardioversion
Author: Aaron Lessen, M.D. Educational Pearls Atrial fibrillation is common. One of the best treatments for a fib is cardioversion back into sinus rhythm. Cardioversion may increase stroke risk if A-Fib duration is greater than 48 hours, but some new data suggests that this risk may happen as soon as 12 hours. However, newer studies show that cardioversion is generally safe as a treatment for A-Fib. References: Aatish Garg, Monica Khunger, Sinziana Seicean, Mina K. Chung, Patrick J.Tchou Incidence of Thromboembolic Complications Within 30 Days of Electrical Cardioversion Performed Within 48 Hours of Atrial Fibrillation Onset. JACC: Clinical Electrophysiology Aug 2016, 2 (4) 487-494; DOI: 10.1016/j.jacep.2016.01.018
Podcast #219: History of Sepsis
Author: Chris Holmes, M.D. Educational Pearls "Sepo' is a term from Homer (author of The Iliad and The Odyssey), and means "I rot". Hippocrates in 400 BC identified sepsis as a "dangerous decay within the body". Galen in 200 AD believed pus was "laudable". The Greeks and Romans used the term "myasma" to describe the smell of swamp and rotting flesh. Dr. Emmanuel Rivers in Detroit did one of the the first big studies about sepsis and was an advocate for goal-directed therapy. Now, Vitamin C cocktails are in use, but new sepsis treatments should be investigated carefully before implementation. References: Funk, Duane J. et al. Sepsis and Septic Shock: A History. Critical Care Clinics , Volume 25 , Issue 1 , 83 - 101

Podcast #218: Estimating Pediatric Weight
Author: Aaron Lessen, M.D. Educational Pearls Asking parents and Broselow Tape are common options for estimating pediatric weight. Equipment sizes should not be adjusted for under/overweight kids based on Broselow Tape estimates. The finger counting method (see reference) is just as accurate as Broselow Tape method, according to one study. References: http://handtevy.com/images/Casestudies/Americanjournalofemergencymedicine.pdf

Podcast #217: Designer Drugs
Author: John Winkler, M.D. Educational Pearls: Designer, or "synthetic" drugs include bath salts, synthetic THC, and many others. Many of these drugs are originally manufactured in China and are shipped globally. Treatment usually involves airway control and sedation - ketamine may be useful. Traditional tox screens do not test for these drugs. References: https://www.drugabuse.gov/related-topics/trends-statistics/national-drug-early-warning-system-ndews

Podcast #216: Roller Coasters and Kidney Stones
Author: Aaron Lessen, M.D. Educational Pearls: Anecdotal evidence suggests that roller coasters may help with kidney stones. A recent study used a model of a kidney and ureter with different sized stones and put it on Thunder Mountain roller coaster in Disney World. There was "dramatic passage" of the kidney stones at the rear of the roller coaster. References: Marc A. Mitchell, DO; David D. Wartinger, DO, JD. Validation of a Functional Pyelocalyceal Renal Model for the Evaluation of Renal Calculi Passage While Riding a Roller Coaster. The Journal of the American Osteopathic Association, October 2016, Vol. 116, 647-652. doi:10.7556/jaoa.2016.128. http://jaoa.org/article.aspx?articleid=2557373

Opioid MIniseries Part IV: Harm Reduction
PRACTICE RECOMMENDATIONS 1. Patients who abuse opioids should be managed without judgement; addiction is a medical condition and not a moral failing. Caregivers should endeavor to meet patients "where they are," infusing empathy and understanding into the patient/medical provider relationship. 2. Every emergency clinician should be well-versed in the safe injection of heroin and other intravenous (IV) drugs, and understand the practical steps for minimizing the dangers of overdose, infection, and other complications. When treating patients with complications of IV drug use, injection habits should be discussed and instruction should be given about safe practices. 3. Emergency department patients who inject drugs should be referred to local syringe access programs, where they can obtain sterile injection materials and support services such as counseling, HIV/hepatitis testing, and referrals. 4. Emergency departments should provide naloxone to high-risk patients at discharge. If the drug is unavailable at the time of release, patients should receive a prescription and be informed about the over-the-counter availability of the drug in most Colorado pharmacies. 5. Emergency clinicians should be familiar with Colorado's regulations pertaining to naloxone. State laws eliminate liability risk for prescribing the drug, encourage good samaritan reporting of overdose, and make naloxone legal and readily available over the counter in most pharmacies. 6. Emergency department patients who receive prescriptions for opioids should be educated on their risks, safe storage methods, and the proper disposal of leftover medications. POLICY RECOMMENDATIONS 1. Harm reduction agencies and community programs that provide resources for people who inject drugs (PWID) should be made readily available. 2. When local programs are unavailable for PWID, emergency departments should establish their own programs to provide services such as safe syringe exchanges.

Opioid Miniseries Part III: Alternative to Opioids
PRACTICE RECOMMENDATIONS 1. All emergency departments should implement ALTO programs and provide opioid-free pain treatment pathways for the following conditions: a. Acute on chronic opioid-tolerant radicular lower back pain b. Opioid-naive musculoskeletal pain c. Migraine or recurrent primary headache d. Extremity fracture or joint dislocation e. Gastroparesis-associated or chronic functional abdominal pain f. Renal colic 2. Emergency departments should integrate ALTO into their computerized physician order entry systems to facilitate a seamless adoption by clinicians. 3. Low-dose, subdissociative ketamine (0.1-0.3 mg/kg) is an effective analgesic that can be opioid-sparing for many acute pain syndromes. Institutional guidelines and policies should be in place to enable clinicians and nurses who administer this agent for pain. 4. For musculoskeletal pain, consider a multimodal treatment approach using acetaminophen, NSAIDs, steroids, topical medications, trigger-point injections, and (for severe pain) ketamine. 5. For headache and migraine, consider a multimodal treatment approach that includes the administration of antiemetic agents, NSAIDs, steroids, valproic acid, magnesium, and triptans. Strongly consider cervical trigger-point injection. 6. For pain with a neuropathic component, consider gabapentin. 7. For pain with a tension component, consider a muscle relaxant. 8. For pain caused by renal colic, consider an NSAID, lidocaine infusion, and desmopressin nasal spray. 9. For chronic abdominal pain, consider low doses of haloperidol, diphenhydramine, and lidocaine infusion. 10. For extremity fracture or joint dislocation, consider the immediate use of nitrous oxide and low-dose ketamine while setting up for ultrasound-guided regional anesthesia. 11. For arthritic or tendinitis pain, consider an intra-articular steroid/anesthetic injection. POLICY RECOMMENDATIONS 1. Hospitals should update institutional guidelines and put policies in place that enable clinicians to order and nurses to administer dose-dependent ketamine and IV lidocaine in non-ICU areas. 2. Emergency departments are encouraged to assemble an interdisciplinary pain management team that includes clinicians, nurses, pharmacists, physical therapists, social workers, and case managers. 3. Reimbursement should be available for any service directly correlated to pain management, the reduction of opioid use, and treatment of drug-addicted patients.

Opioid Miniseries Part II: Limiting Opioids in the Emergency Department
RACTICE RECOMMENDATIONS 1. Opioids are inherently dangerous, highly addictive drugs with significant abuse potential, numerous side effects, lethality in overdose, rapid development of tolerance, and debilitating withdrawal symptoms. They should be avoided whenever possible and, in most cases, initiated only after other modalities of pain control have been trialed. 2. Prior to prescribing an opioid, physicians should perform a rapid risk assessment to screen for abuse potential and medical comorbidities. Alternative methods of pain control should be sought for patients at increased risk for abuse, addiction, or adverse reactions. 3. Emergency physicians should frequently consult Colorado's prescription drug monitoring program (PDMP) to assess a patient's history of prescription drug abuse, misuse, or diversion. 4. Emergency physician groups should strongly consider tracking, collecting, and sharing individual opioid prescribing patterns with their clinicians to decrease protocol variabilities. 5. Strongly consider removing prepopulated doses of opioids from order sets in computerized provider order entry (CPOE) systems. 6. Opioid alternatives and nonpharmacological therapies should be used to manage patients with acute low back pain, in whom opioids are particularly detrimental. Opioids should be prescribed only after alternative treatments have failed. 7. Potential drug interactions must be evaluated, and opioids should be avoided in patients already taking benzodiazepines, barbiturates, or other narcotics. 8. Patients with chronic pain should receive opioid medications from one practice, preferably their primary care provider or pain specialist. Opioids should be avoided in the emergency department treatment of most chronic conditions. Emergency physicians should coordinate care with a patient's primary care or pain specialist whenever possible, and previous patient-physician contracts regarding opioid use should be honored. 9. Clinicians should abstain from adjusting opioid dosing regimens for chronic conditions and avoid routinely prescribing opioids for acute exacerbations of chronic noncancer pain. 10. "Long-acting" or "extended-release" opioid products should be avoided for the relief of acute pain. 11. Patients receiving controlled medication prescriptions should be able to verify their identity. 12. Patients who receive opioids should be educated about their side effects and potential for addiction, particularly when being discharged with an opioid prescription. 13. When considering opioids, clinicians should prescribe the lowest possible effective dose in the shortest appropriate duration (eg, 14. Emergency departments should refuse to refill lost or stolen opioid prescriptions. POLICY RECOMMENDATIONS 1. As has been done in other states, the Colorado PDMP should develop an automated query system that can be more readily integrated into electronic health records and accessed by emergency clinicians. 2. Pain control should be removed from patient satisfaction surveys, as they may unfairly penalize physicians for exercising proper medical judgement. 3. Opioid prepacks should be avoided or eliminated in the emergency department if 24-hour pharmacy support is available. 4. Pain should not be considered the "fifth vital sign."

Opioid Miniseries Part I: Medicine's Greatest Folly
The Emergency Medical Minute proudly presents an educational podcast series sponsored by the Colorado Hospital Association addressing our the United States' opioid epidemic.

Podcast #215: Ankle Pain
Author: Donald Stader, M.D. Educational Pearls: The most common ankle injury mechanism is an inversion. Most common broken bone in the ankle is the fibula. During exam, it is important to palpate over the fibular head, medial and lateral malleoli, over the 5th metatarsal and over the cuboid bone. If no tenderness in these areas and the patient is walking - they have a sprain and can be sent home without imaging. In calcaneal fractures, make sure to image the lumbar spine since up to 30% of calcaneal fractures are associated with lumbar spine injury. References: http://orthosurg.ucsf.edu/oti/patient-care/divisions/sports-medicine/physical-examination-info/ankle-physical-examination/

Podcast #214: Dizziness
Author: Aaron Lessen, M.D. Educational Pearls: We can differentiate verto into benign problems such as vestibular problem (peripheral problem), or something more worrisome that originates in the brain (central problem). Dizziness + other symptoms makes us think about origination in the CNS. Symptoms include Dizziness, Diplopia, Dysarthria, Dysphagia, Dysmetria. References: http://www.medicalnewstoday.com/knowledge/160900/vertigo-causes-symptoms-treatments http://www.mayoclinic.org/diseases-conditions/dizziness/basics/causes/con-20023004