Emergency Medical Minute
1,164 episodes — Page 16 of 24

Podcast #387: Fluoroquinolones are Perfectly Safe?
Author: Don Stader, MD Educational Pearls: Fluoroquinolones can cause connective tissue disruption leading not only to tendon rupture but also aortic dissection Retrospective study from Taiwan showed over a 2x higher rate of dissection when exposed to fluoroquinolones (1.6% vs 0.6%) Remember to think about aortic dissection when you have a patient with chest pain that travels and/or involves neurologic symptoms Try to use fluoroquinolones when no other appropriate antibiotic exists as they have significant other side effects as well Editor's note: In July 2018, the FDA required strengthening of warning labels on fluoroquinolones about the risks of mental health effects and hypoglycemia References: Lee CC, Lee MG, Hsieh R, Porta L, Lee WC, Lee SH, Chang SS. Oral Fluoroquinolone and the Risk of Aortic Dissection. J Am Coll Cardiol. 2018 Sep 18;72(12):1369-1378. doi: 10.1016/j.jacc.2018.06.067. PubMed PMID: 30213330. Khaliq Y, Zhanel GG. Fluoroquinolone-associated tendinopathy: a critical review of the literature. Clin Infect Dis. 2003 Jun 1;36(11):1404-10. Epub 2003 May 20. Review. PubMed PMID: 12766835. https://www.fda.gov/downloads/Drugs/DrugSafety/UCM612834.pdf Summary by Travis Barlock, MS4 | Edited by Erik Verzemnieks, MD

Podcast #386: Respecting Transgender Patients
Author: Kasey Champion, MD Educational Pearls: Transgender populations are frequent victims of discrimination in healthcare Ask transgender patients what their preferred pronoun is It is sometimes important to ask about transition status (i.e. on hormones, surgery) References: Chisolm-Straker M, Willging C, Daul AD, McNamara S, Sante SC, Shattuck DG 2nd, Crandall CS. Transgender and Gender-Nonconforming Patients in the Emergency Department: What Physicians Know, Think, and Do. Ann Emerg Med. 2018 Feb;71(2):183-188.e1. doi: 10.1016/j.annemergmed.2017.09.042. Epub 2017 Nov 3. PubMed PMID: 29103796.

Podcast #385: Probiotics
Author: John Winkler, MD Educational Pearls: Probiotics are bacteria that are ingested to promote gut health but recent research casts doubt on their effectiveness. Recent study suggests that most probiotics that are ingested are killed by stomach acid. Those that remain are not very healthy and are outcompeted by the normal gut flora. Probiotics should not be given as a one-size-fits-all treatment. References: Zmora N, Zilberman-Schapira G, Suez J, Mor U, Dori-Bachash M, Bashiardes S, Kotler E, Zur M, Regev-Lehavi D, Brik RB, Federici S, Cohen Y, Linevsky R, Rothschild D, Moor AE, Ben-Moshe S, Harmelin A, Itzkovitz S, Maharshak N, Shibolet O, Shapiro H, Pevsner-Fischer M, Sharon I, Halpern Z, Segal E, Elinav E. Personalized Gut Mucosal Colonization Resistance to Empiric Probiotics Is Associated with Unique Host and Microbiome Features. Cell. 2018 Sep 6;174(6):1388-1405.e21. doi: 10.1016/j.cell.2018.08.041. PubMed PMID: 30193112.

Podcast #384: Don't stab a PTA?
Author: Don Stader, MD Educational Pearls: Recent study suggests we may not need to drain uncomplicated peritonsillar abscesses Patients who received medical therapy alone had no difference in complications and failure compared to those who received surgical drainage plus medical therapy Medical therapy in study was ceftriaxone, clindamycin, and dexamethasone Medical therapy was also associated with fewer opioid prescriptions, sore days, and days off from work. References: Battaglia A, Burchette R, Hussman J, Silver MA, Martin P, Bernstein P. Comparison of Medical Therapy Alone to Medical Therapy with Surgical Treatment of Peritonsillar Abscess. Otolaryngol Head Neck Surg. 2018 Feb;158(2):280-286. doi: 10.1177/0194599817739277. Epub 2017 Nov 7. PubMed PMID: 29110574.

Podcast #383: Prehospital Tubes
Author: Sam Killian, MD Educational Pearls: Two high quality randomized control trials published in 2018 demonstrated no difference in mortality or neurologic outcomes when using a supraglottic airway compared to endotracheal intubation in out of hospital cardiac arrest These two trials enrolled over a combined 12000 patients Supraglottic airways have a higher success rate than intubations References: Benger JR, Kirby K, Black S, Brett SJ, Clout M, Lazaroo MJ, Nolan JP, Reeves BC, Robinson M, Scott LJ, Smartt H, South A, Stokes EA, Taylor J, Thomas M, Voss S, Wordsworth S, Rogers CA. Effect of a Strategy of a Supraglottic Airway Device vs Tracheal Intubation During Out-of-Hospital Cardiac Arrest on Functional Outcome: The AIRWAYS-2 Randomized Clinical Trial. JAMA. 2018 Aug 28;320(8):779-791. doi: 10.1001/jama.2018.11597. PubMed PMID: 30167701 Wang HE, Schmicker RH, Daya MR, Stephens SW, Idris AH, Carlson JN, Colella MR, Herren H, Hansen M, Richmond NJ, Puyana JCJ, Aufderheide TP, Gray RE, Gray PC, Verkest M, Owens PC, Brienza AM, Sternig KJ, May SJ, Sopko GR, Weisfeldt ML, Nichol G. Effect of a Strategy of Initial Laryngeal Tube Insertion vs Endotracheal Intubation on 72-Hour Survival in Adults With Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA. 2018 Aug 28;320(8):769-778. doi: 10.1001/jama.2018.7044. PubMed PMID: 30167699.

Podcast #382: Shoulder Separations
Author: Ryan Circh, MD Educational Pearls: A "shoulder separation" is when the clavicle separates from the scapula - also referred to as an acromio-clavicular (AC) separation Diagnosis is clinical: pain over AC joint, pain with adduction, and difficulty raising harm past horizontal Early range of motion can be critical for recovery References: Lemos MJ. The evaluation and treatment of the injured acromioclavicular joint in athletes. Am J Sports Med. 1998 Jan-Feb;26(1):137-44. Review. PubMed PMID: 9474415. Monica J, Vredenburgh Z, Korsh J, Gatt C. Acute Shoulder Injuries in Adults. Am Fam Physician. 2016 Jul 15;94(2):119-27. Review. PubMed PMID: 27419328.
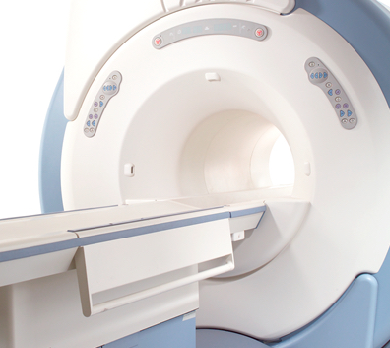
Podcast #381: MRI... Burns?
Author: Sam Killian, MD Educational Pearls: MRI machines can generate enough heat from the radiofrequency to cause thermal burns Patients with EKG stickers, medication patches, clothing impregnated with metallic ions, etc., can all increase risk of burns Even skin-to-skin contact within the patient can cause a misinterpretation from the software and increased energy, leading to burn References: Cross NM, Hoff MN, Kanal KM. Avoiding MRI-Related Accidents: A Practical Approach to Implementing MR Safety. J Am Coll Radiol. 2018 Aug 24. pii: S1546-1440(18)30762-2. doi: 10.1016/j.jacr.2018.06.022. [Epub ahead of print] PubMed PMID: 30149951. Takahashi T, Fujimoto N, Hamada Y, Tezuka N, Tanaka T. MRI-related thermal injury due to skin-to-skin contact. Eur J Dermatol. 2016 Jun 1;26(3):296-8. doi: 10.1684/ejd.2016.2740. PubMed PMID: 26987101. Pietryga JA, Fonder MA, Rogg JM, North DL, Bercovitch LG. Invisible metallic microfiber in clothing presents unrecognized MRI risk for cutaneous burn. AJNR Am J Neuroradiol. 2013 May;34(5):E47-50. doi: 10.3174/ajnr.A2827. Epub 2011 Dec 15. PubMed PMID: 22173750. Dempsey MF, Condon B. Thermal injuries associated with MRI. Clin Radiol. 2001 Jun;56(6):457-65. Review. PubMed PMID: 11428795.

Podcast #380: Oxygen for the kill
Author: Ryan Circh, MD Educational Pearls: Review of 25 randomized control trials encompassing 16,037 acutely ill hospitalized patients Patients given oxygen with saturations > 94% on room air were found to have associated increased mortality in-hospital, at 30-days, and at long-term follow up It may seem intuitive, but do not give oxygen to patients that do not need it References: Chu DK, et al (2018). Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. Lancet. 391(10131):1693-1705

Podcast #379: Patient Perspectives of the Flu
Author: Sam Killian, MD Educational Pearls: Patients may have certain fears or expectations about the flu based on hearsay and other less reliable sources Taking extra time explaining the risks of the flu may help base these expectations more in reality This includes providing good return precautions and acknowledging that the disease can still be unpredictable

Podcast #378: Is That a Brown Recluse Spider Bite?
Author: Michael Hunt, MD Educational Pearls: Use the mnemonic NOT RECLUSE to rule out a brown recluse spider bite: Numerous bites (recluse spiders will bite once) Occurence (recluse bites between April- October) Timing (recluse spiders are… get this… reclusive) Red (recluse bites are white/pale) Elevated (recluse bites are flat) Chronic (recluse bites are acute) Large (recluse wounds are small) Ulceration, early (recluse bites ulcerate between 7-14 days) Swollen (recluse bites are flat) Exudative (recluse bites are dry) References: Stoecker WV, Vetter RS, Dyer JA. NOT RECLUSE-A Mnemonic Device to Avoid False Diagnoses of Brown Recluse Spider Bites. JAMA Dermatol. 2017 May 1;153(5):377-378. doi: 10.1001/jamadermatol.2016.5665. PubMed PMID: 28199453.

Podcast #377: Endocarditis
Author: Nick Tsipis, MD Educational Pearls: Persistent fever or positive blood cultures should raise suspicion for endocarditis Patients with recent dental procedures, recent cardiac surgeries are at risk, or who inject drugs are at higher risk Physical exam findings may include fever with a new murmur, Janeway lesions, Osler nodes, and/or splinter hemorrhages References: Long B, Koyfman A. Infectious endocarditis: An update for emergency clinicians. Am J Emerg Med. 2018 Sep;36(9):1686-1692. doi: 10.1016/j.ajem.2018.06.074. Epub 2018 Jul 2. Review. PubMed PMID: 30001813. Murdoch DR, Corey GR, Hoen B et. al. International Collaboration on Endocarditis-Prospective Cohort Study (ICE-PCS) Investigators. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch Intern Med. 2009 Mar 9;169(5):463-73. doi: 10.1001/archinternmed.2008.603

Podcast #376: Alcohol Intoxication
Educational Pearls: Blood concentrations over 0.4 mg/dL is associated with respiratory depression and possible death in alcohol naive patients Alcohol overdose accounts to 2,200 deaths per year Don't forget about checking for hypoglycemia in severe alcohol intoxication Consider ketamine for agitation to prevent further respiratory depression Editor's note: check out our podcast on ketamine for alcohol withdrawal here References: Jung YC, Namkoong K. Alcohol: intoxication and poisoning - diagnosis and treatment. Handb Clin Neurol. 2014;125:115-21. doi: 10.1016/B978-0-444-62619-6.00007-0. Centers for Disease Control and Prevention (CDC). "Vital signs: binge drinking prevalence, frequency, and intensity among adults-United States, 2010." MMWR. Morbidity and mortality weekly report 61.1 (2012): 14.
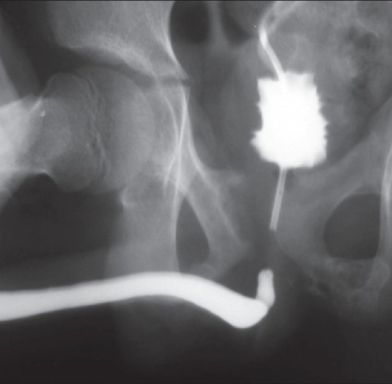
Podcast #375: Retrograde Urethrogram
Author: Jared Scott, MD Educational Pearls: Blood at urethral meatus in trauma can be a sign of bladder/urethral injury Blind placement of a Foley catheter can make an undiagnosed urethral injury worse Urethral injury is evaluated using a retrograde urethrogram (RUG) If urethra is confirmed to be intact, Foley catheter can be placed to allow additional tests References: Avery, L. (2012). Imaging of male pelvic trauma. Radiologic Clinics of North America., 50(6), 1201-1217.

Podcast #374: Iliac Artery Endofibrosis
Author: Sue Chilton, MD Educational Pearls: An unusual cause of leg pain that can mimic sciatica/claudication Predominantly occurring in high endurance athletes, particularly cyclists and runners More common in men Check supine ABIs 1 minute after activity in the ED: a value References: Mansour A, Murney S, Jordan K, Laperna L. Endofibrosis: an unusual cause of leg pain in an athlete. J Sports Med Phys Fitness. 2016 Jan-Feb;56(1-2):157-61. Epub 2015 Jul 3. PubMed PMID: 26140352. Peach G, Schep G, Palfreeman R, Beard JD, Thompson MM, Hinchliffe RJ. Endofibrosis and kinking of the iliac arteries in athletes: a systematic review. Eur J Vasc Endovasc Surg. 2012;43(2):208–17.

Podcast # 373: Legionnaires Disease
Author: Gretchen Hinson, MD Educational Pearls: Legionnaires disease refers to a severe pneumonia caused by Legionella pneumophilia and occurs typically at the extremes of age Associated gastrointestinal symptoms (nausea/vomiting/diarrhea) may be present Hyponatremia is a common laboratory finding Legionella urinary antigen can be a convenient test to identify the infection Treatment is with fluoroquinolones, macrolides and/or tetracyclines References Pierre DM, Baron J, Yu VL, Stout JE. Diagnostic testing for Legionnaires' disease. Annals of Clinical Microbiology and Antimicrobials. 2017;16:59. doi:10.1186/s12941-017-0229-6. Cunha BA, Cunha CB. Legionnaire's Disease and its Mimics: A Clinical Perspective. Infect Dis Clin North Am. 2017 Mar;31(1):95-109. doi: 10.1016/j.idc.2016.10.008. Review.

Podcast # 372: The Latest on Epinephrine in Cardiac Arrest
Author: Don Stader, MD Educational Pearls: 8014 patients with out-of-hospital cardiac arrest randomized to epinephrine vs placebo 30-day survival was not dramatically better between groups (3.2%in the epinephrine group and 2.4% in the placebo group) Functional neurological outcome was nearly identical at 2.2% and 1.9% of patients Adds to literature that epinephrine provides little important benefit in cardiac arrest - focus on chest compressions and early defibrillation Editor's note: NNT for epinephrine to prevent one death in this study was 115 - compared to bystander CPR (NNT 15) and defibrillation (NNT 5) from prior studies. References Perkins GD et. al. . A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. N Engl J Med. 2018 Aug 23;379(8):711-721. doi: 10.1056/NEJMoa1806842. Epub 2018 Jul 18. Kitamura T, Kiyohara K, Sakai T, et al. Public-access defibrillation and out-of-hospital cardiac arrest in Japan. N Engl J Med 2016;375:1649-1659. Hasselqvist-Ax I, Riva G, Herlitz J, et al. Early cardiopulmonary resuscitation in out-of-hospital cardiac arrest. N Engl J Med 2015;372:2307-2315. Hagihara A, Hasegawa M, Abe T, Nagata T, Wakata Y, Miyazaki S. Prehospital epinephrine use and survival among patients with out-of-hospital cardiac arrest. JAMA. 2012 Mar 21;307(11):1161-8. doi: 10.1001/jama.2012.294. PubMed PMID: 22436956. Sanghavi P, Jena AB, Newhouse JP, Zaslavsky AM. Outcomes after out-of-hospital cardiac arrest treated by basic vs advanced life support. JAMA Intern Med. 2015 Feb;175(2):196-204. doi: 10.1001/jamainternmed.2014.5420.

Podcast # 371: EKG changes of Hyperkalemia
Author: Jared Scott, MD Educational Pearls: EKG changes do not necessarily correlate to degree of hyperkalemia Traditional progression through peaked T-waves, flattened p-waves, QRS widening, and then sine-waves before asystole References Mattu A, Brady WJ, Robinson DA. Electrocardiographic manifestations of hyperkalemia. Am J Emerg Med. 2000;18:721–729.

Podcast # 370: Rapid Fire Neonatal Resuscitation
Author: Erik Verzemnieks, MD Educational Pearls: In the panic of a precipitous ED delivery, remember: Warm. Dry. Stim. It will solve most of your problems in most scenarios Start compressions if heart rate is less than 60 Put the pulse ox on the right hand - it may make a difference as it is preductal Editor's note: detecting a heart rate can be tough in a newborn - you can feel the umbilical stump or just listen with your stethoscope References Gary Weiner & Jeanette Zaichkin. Textbook of Neonatal Resuscitation (NRP), 7th Ed, 2016. American Academy of Pediatrics & American Heart Association.

Podcast # 369: Five powerful toxins - the definitive list?
Author: Michael Hunt, MD Educational Pearls: Here is a list of some very toxic natural substances: #5: Tetrodotoxin: Found in pufferfish and other aquatic species #4: Ricin: made from castor beans #3: Mercury: natural element absorbable through skin and gloves #2: Batrachotoxin: found on poison dart frogs #1: Botulinum toxin: produced by Clostridium botulinum and causes a descending paralysis Editor's note: batrachotoxin is thought to be accumulated by the beatles and other insects dart frogs eat - those in captivity therefore are not poisonous References https://theconversation.com/handle-with-care-the-worlds-five-deadliest-poisons-56089

Podcast # 368: Prehospital Plasma
Author: Aaron Lessen, MD Educational Pearls: Non-blinded randomized study assessing 30-day mortality benefit from plasma-first resuscitation in patients at risk hemorrhagic shock Study involved aeromedical transport of trauma patients 30-day mortality 23.2 % in intervention group vs. 33.0% in standard care group Editor's note: a similar study published in Lancet at the same time showed no mortality benefit from prehospital administration of plasma in a slightly different population which had much shorter ground transport times a major trauma center References Sperry JL, Guyette FX, Brown JB, Yazer MH, Triulzi DJ, Early-Young BJ, Adams PW, Daley BJ, Miller RS, Harbrecht BG, Claridge JA, Phelan HA, Witham WR, Putnam AT, Duane TM, Alarcon LH, Callaway CW, Zuckerbraun BS, Neal MD, Rosengart MR, Forsythe RM, Billiar TR, Yealy DM, Peitzman AB, Zenati MS; PAMPer Study Group.. Prehospital Plasma during Air Medical Transport in Trauma Patients at Risk for Hemorrhagic Shock. N Engl J Med. 2018 Jul 26;379(4):315-326. doi: 10.1056/NEJMoa1802345.

Podcast # 367: Digital Necrosis after Epinephrine Drip
Podcast # 367: Digital Necrosis after Epinephrine Drip Author: Jared Scott, MD. Educational Pearls: Make sure to monitor for limb ischemia in all patients on vasopressors Good reminder that vasopressors are not risk free - use them only on patients that need them! References Daroca-Pérez, R., & Carrascosa, M. F. . Digital necrosis: a potential risk of high-dose norepinephrine. Therapeutic Advances in Drug Safety. 2017. 8(8), 259–261. http://doi.org/10.1177/2042098617712669.

Podcast # 366: Ehlers Danlos
Podcast # 366: Ehlers Danlos Author: Gretchen Hinson, MD. Educational Pearls: Heritable mutation in collagen synthesis and expression commonly resulting in joint hyperextension and skin elasticity. Vascular type can result in aneurysm formation and rupture in young patients. Patients are also at risk for spontaneous bowel rupture. Pregnant women can present with uterine rupture. References Byers PH, Murray ML (2012). "Heritable collagen disorders: the paradigm of Ehlers–Danlos syndrome". Journal of Investigative Dermatology. 132 (E1): E6–11. Pepin MG, Byers PH. Ehlers-Danlos Syndrome Type IV. In: Pagon RA, Bird TD, Dolan CR, et al., eds. GeneReviews [Internet]. Seattle (WA): University of Washington, Seattle; 1993-. Yoneda, A., Okada, K., Okubo, H., Matsuo, M., Kishikawa, H., Naing, B. T., … Shimada, T. (2014). Spontaneous Colon Perforations Associated with a Vascular Type of Ehlers-Danlos Syndrome. Case Reports in Gastroenterology, 8(2), 175–181. http://doi.org/10.1159/000363373

Podcast # 365: Renal Trigger Point Injections
Author: Erik Verzemnieks, MD Educational Pearls: Single study in Japan demonstrated possible effectiveness of renal colic trigger point Patients had injection at the area of maximal tenderness on palpation of the flank Compared to a muscle relaxer, injection of local anesthetic at the trigger point had faster time to pain relief and fewer rescue therapies References Iguchi, M et al. Randomized trial of trigger point injection for renal colic. International Journal of Urology. 2002. 9(9): 475-479
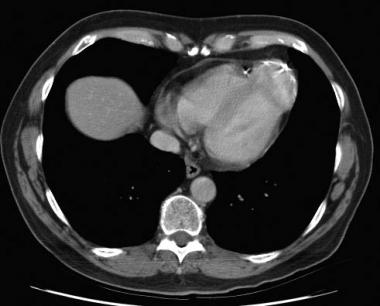
Podcast # 364: Other causes of ST elevation
Author: Peter Bakes, MD Educational Pearls: Pericarditis, LBBB, LVH and left ventricular aneurysms can all present with ST elevation. Ventricular aneurysm will present days after a cardiac event with ST elevation and Q waves in the affected leads. Ventricular aneurysms may cause papillary muscle dysfunction with a resultant holosystolic murmur and even heart failure. References Victor F. Froelicher; Jonathan Myers (2006). Exercise and the heart. Elsevier Health Sciences. pp. 138–. ISBN 978-1-4160-0311-3. Nagle RE, Williams DO. (1974) Proceedings: Natural history of ventricular aneurysm without surgical treatment. British Heart Journal, 36:1037.

Podcast # 363: Ketamine for Alcohol Withdrawal
Educational Pearls: Recent study has shown adjunctive ketamine can be useful in setting of alcohol withdrawal. Ketamine was associated with a decrease in the amount of benzodiazepines needed, likelihood of intubation, and a decrease in ICU length of stay by 3 days. For patients with benzodiazepine resistance, ketamine was shown to have symptom relief in an hour and decreased rate of benzodiazepine infusion. References Pizon A, Lynch M, Benedict N, et al. 2018. Adjunct Ketamine Use in the Management of Severe Ethanol Withdrawal. Critical Care Medicine. 46(8):e768-e771. Shah, P., McDowell, M., Ebisu, R. et al. J. Med. Toxicol. (2018). https://doi.org/10.1007/s13181-018-0662-8

Podcast # 362: Giant Hogweed
Author: John Winkler, MD Educational Pearls: Tall flowering plant with phototoxic sap Direct skin contact with the sap can cause the skin to become photosensitive Severe blisters and even burns can result References Diebel, Matthew (18 June 2018). "Giant Hogweed, a Plant That Can Cause Burns and Blindness, Found in Virginia". USA Today.

Podcast # 361: Vertiginous Dizziness
Author: Peter Bakes, MD Educational Pearls: Important to find out if patients mean dysequilibrium, lightheadedness, or vertigo when patients say they are "dizzy." Differentiate central vs. peripheral vertigo Central vertigo typically present with bulbar syndromes (difficulty swallowing, facial nerve palsy) and cerebellar symptoms (ataxia). Peripheral vertigo typically present with sudden onset vertigo with nausea and vomiting in the absence of bulbar symptoms. Episodic? BPPV or Meniere's Disease. BPPV has not auditory symptoms and is associated with head position; Meniere's has hearing loss, tinnitus, and ear fullness. Constant? Neuronitis has no auditory symptoms, while labyrinthitis has associated hearing loss/tinnitus and is associated with a recent infection (OM). References Baloh RW. Differentiating between peripheral and central causes of vertigo. Otolaryngol Head Neck Surg 1998; 119:55. Chase M, Goldstein JN, Selim MH, et al. A prospective pilot study of predictors of acute stroke in emergency department patients with dizziness. Mayo Clin Proc 2014; 89:173. Kerber KA, Brown DL, Lisabeth LD, et al. Stroke among patients with dizziness, vertigo, and imbalance in the emergency department: a population-based study. Stroke 2006; 37:2484.
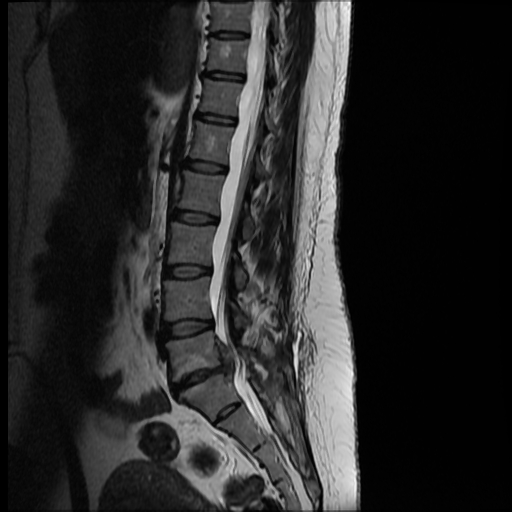
Podcast # 360: Epidural Abscess Screening
Author: Dylan Luyten, MD. Educational Pearls: Dangerous causes of back pain: AAA, cauda equina syndrome, epidural abscess. Young person with back pain needs to be evaluated for injection drug use (major risk factor). Patient with focal neurologic deficits (FND) require an MRI. Patients without FND can be screened with ESR and CRP. An ESR Treatment is IV antibiotics and surgical debridement. References Davis DP et al. Prospective evaluation of a clinical decision guideline to diagnose spinal epidural abscess in patients who present to the emergency department with spine pain, Journal of Neurosurgery: Spine. 2011. 14:765-770.
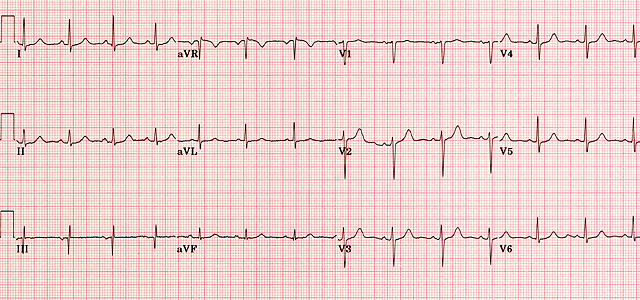
Podcast # 359: Normal EKG
Author: Sam Killian, MD. Educational Pearls: Computer interpretation has a very good negative predictive value of a normal EKG (99%). Of 222 interpreted as "normal," 13 were deemed to have some abnormality by a cardiologist in a recent study. Those 13 EKG's were read by 2 ER docs, and only 1 missed interpretation warranted a move from triage to a bed. References Katie E. Hughes KE., Scott M. Lewis SM., Laurence Katz and Jonathan Jones Safety of Computer Interpretation of Normal Triage Electrocardiograms. 2017. Academic Emergency Medicine 24(1):120-124. http://onlinelibrary.wiley.com/doi/10.1111/acem.13067/full.
Podcast # 358: Affordable ear drop alternatives
Author: Erik Verzemnieks, MD Educational Pearls: Otic (ear) specific antibiotic drops can be expensive Opthalmic (eye) versions are basically identical and can be used as an affordable substitute as many are on the $4 drug lists But don't do the reverse (don't use ear drops on the eye) Use caution when administering aminoglycoside if tympanic membrane rupture is present References https://tgtfiles.target.com/pharmacy/WCMP02-032536_RxGenericsList_NM7.pdf http://i.walmart.com/i/if/hmp/fusion/four_dollar_drug_list.pdf https://www.uptodate.com/contents/external-otitis-treatment

Podcast #357: Local Anesthetic Toxicity
Author: Michael Hunt, MD Educational Pearls: Toxicity happens from local anesthetics being given too fast, too much, or in the unintended spot Systemic toxicity manifests first with neurologic symptoms like circumoral numbness, tinnitus, blurred vision, nausea, and even seizures. Severe toxicity can then progress to arrhythmias and cardiac arrest. Maximum doses of lidocaine: 4 mg/kg; and with epinephrine: 7mg/kg. Maximum dose of bupivacaine: 2mg/kg; with epinephrine 3mg/kg Editor note: treat seizures with benzodiazepines and avoid propofol for sedation; severe toxicity can also be treated with a 20% lipid emulsion, though there is debate on its efficacy References Dickerson DM, Apfelbaum JL. Local anesthetic systemic toxicity. Aesthet Surg J. 2014 Sep;34(7):1111-9. doi: 10.1177/1090820X14543102. Neal JM, Mulroy MF, Weinberg GL; American Society of Regional Anesthesia and Pain Medicine.. American Society of Regional Anesthesia and Pain Medicine checklist for managing local anesthetic systemic toxicity: 2012 version. Reg Anesth Pain Med. 2012 Jan-Feb;37(1):16-8. doi: 10.1097/AAP.0b013e31822e0d8a. Vasques F, Behr AU, Weinberg G, Ori C, Di Gregorio G. A Review of Local Anesthetic Systemic Toxicity Cases Since Publication of the American Society of Regional Anesthesia Recommendations: To Whom It May Concern. Reg Anesth Pain Med. 2015 Nov-Dec;40(6):698-705. doi: 10.1097/AAP.0000000000000320.

Podcast # 356: Babies can't be born addicted
Author: Don Stader, MD. Educational Pearls: A baby can be born dependent on opioids but not addicted to them. Opioid addiction (Opioid Use Disorder) is a disease of mature brains and is characterized by compulsive drug use despite adverse consequences. Opioid addiction is a disease that affects the reward center of the brain Pregnant patients struggling with addiction do better when started on buprenorphine or methadone. This treatment will cause opioid withdrawal syndrome in newborns, but not the long term morbidity and mortality of illicit opioids. References Gowing L, Farrell MF, Bornemann R, Sullivan LE, Ali R. Oral substitution treatment of injecting opioid users for prevention of HIV infection. Cochrane Database of Systematic Reviews 2011, Issue 8: CD004145. DOI: 10.1002/14651858.CD004145.pub4. Volkow ND, Koob GF, McLellan AT ( 2016). "Neurobiologic Advances from the Brain Disease Model of Addiction." New England Journal of Medicine. 374 (4): 363–371.

Podcast #355: Syphilis
Author: Aaron Lessen, MD Educational Pearls: Re-emerging STI. Progresses through distinct phases if untreated: Primary syphilis: frequently overlooked because initial chancre is painless. Secondary syphilis: viral syndrome, rash on trunk, palms, and soles. Latent syphilis: asymptomatic period, lasting 5-20 years. Tertiary syphilis: includes neurosyphilis (dementia, encephalitis, etc.) and cardiovascular syphilis (aortitis, etc). Treatment penicillin G 2.4 million units once for primary or secondary treatment; once weekly for 3 weeks for latent/tertiary. References Mattei, P., Beachkofsky, T., Gilson, R., Wisco, O. Syphilis: A reemerging infection. 2012. American Family Physician., 86(5), 433-440.

Podcast # 354: Hematometra
Author: Sam Killian, MD Educational Pearls: Hematometra: uterus filled with blood due to obstruction of outflow tract. Most commonly a result congenital abnormalities (imperforate hymen, transverse vaginal septum, etc.) but can be acquired due to cervical stenosis, intrauterine adhesions, neoplasms, and post-surgical scarring. Symptoms include: pain, abnormal bleeding, enlarged uterus Diagnosis: commonly achieved by ultrasound and physical exam. Treatment is surgical (cervical dilatation, hysteroscopy, etc.). References U Nayak A, Swarup A, G S J, N S. Hematometra and acute abdomen. Journal of Emergencies, Trauma and Shock. 2010;3(2):191-192. doi:10.4103/0974-2700.62117. Kotter HC, Weingrow D, Canders CP. Hematometrocolpos in a Pubescent Girl with Abdominal Pain. Clinical Practice and Cases in Emergency Medicine. 2017;1(3):218-220. doi:10.5811/cpcem.2017.3.33369.

Podcast # 353: Xofluza
Author: Sam Killian, MD Educational Pearls: Japan recently approved baloxavir marboxil (Xofluza), which may potentially "kill" Flu A/B within 24 hours Recent RCT trial showed superiority over oseltamavir (Tamiflu) in cessation of viral shedding (24 vs 72 hours) Compared to placebo, superior in time to symptom resolution (53.7 vs 80.7 hours) Administered as single dose Yet to be considered for FDA approval References Portsmouth S, Kawaguchi K, Arai M, Tsuchiya K, Uehara T. Cap-dependent Endonuclease Inhibitor S-033188 for the Treatment of Influenza: Results from a Phase 3, Randomized, Double-Blind, Placebo- and Active-Controlled Study in Otherwise Healthy Adolescents and Adults with Seasonal Influenza. Open Forum Infectious Diseases. 2017;4(Suppl 1):S734. doi:10.1093/ofid/ofx180.001.

Podcast #352: TXA for Epistaxis
Podcast #352: TXA for Epistaxis Author: Chris Holmes, M.D. Educational Pearls: TXA: tranexamic acid; used in control of bleeding in major trauma, postpartum hemorrhage, etc. In study of 216 patients with epistaxis, TXA placed on a pledget was compared to anterior cotton nasal packing. The TXA group had faster time to bleeding control, quicker time to discharge, better patient satisfaction, and lower rates of re-bleeding. References: Zahed R, Moharamzadeh P, Alizadeharasi S, Ghasemi A, Saeedi M. A new and rapid method for epistaxis treatment using injectable form of tranexamic acid topically: a randomized controlled trial. Am J Emerg Med. 2013 Sep;31(9):1389-92. doi: 10.1016/j.ajem.2013.06.043.
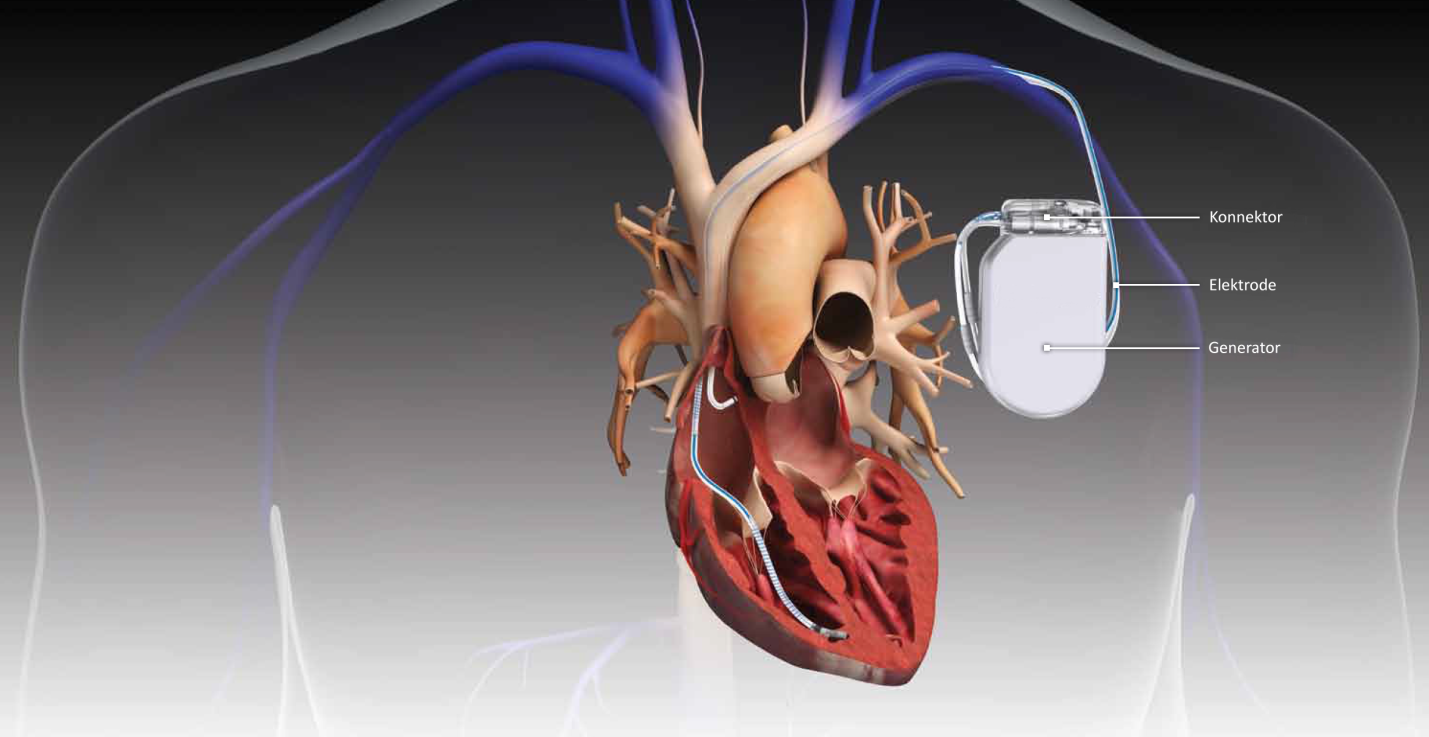
Podcast #351: Indications for AICD
Author: Pete Bakes, MD Educational Pearls: AICD: Automated Implantable Cardioverter-Defibrillator. Can be placed for secondary prevention of cardiac arrest (i.e. history of cardiac arrest not from reversible cause). Also indications for primary prevention: EF 35% or less; ventricular tachycardia with underlying structural heart disease; Brugada; genetic-induced prolonged QT-syndromes. References: Al-Khatib SM et. al. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm. 2017 Oct 30. pii: S1547-5271(17)31249-3. doi: 10.1016/j.hrthm.2017.10.035.

Podcast # 350: Pressors and Ischemia
Author: Nick Hatch, MD. Educational Pearls: A common concern using vasopressors is the risk of digital and mesenteric ischemia. The absolute risk of digital ischemia and/or mesenteric ischemia is pretty low. Norepinephrine at its highest doses carries a 5% digital ischemia rate and a 2% mesenteric ischemia rate. The studies demonstrating this complication were predominately patients with pre-existing liver disease. Providers commonly mistake purpura fulminans, a common complication of sepsis, for digital ischemia. References Brown, SM. et al. Survival After Shock Requiring High-Dose Vasopressor Therapy. Chest. 2013. 143(3), 664–671. http://doi.org/10.1378/chest.12-1106. Malay MB et al. Heterogeneity of the vasoconstrictor effect of vasopressin in septic shock. Critical Care Medicine. 2004. 32(6), 1327-31.

Podcast # 349: Fat Emboli
Author: Sue Chilton, MD Educational Pearls: Triad of fat emboli syndrome is a petechial rash, AMS, and respiratory distress. Petechiae usually start in the axilla. 90% of patients with long bone fractures will shed fat. May see ground-glass opacities on imaging, but perfusion defects will not be seen on CTA or V/Q scan Patients with a PFO can have cerebral involvement. References Newbigin K, Souza CA, Torres C, Marchiori E, Gupta A, Inacio J, Armstrong M, Peña E. Fat embolism syndrome: State-of-the-art review focused on pulmonary imaging findings. Respir Med. 2016.113:93-100. doi: 10.1016/j.rmed.2016.01.018. Kosova E, Bergmark B, Piazza G. Fat embolism syndrome. Circulation. 2015. 20;131(3):317-20. doi: 10.1161/CIRCULATIONAHA.114.010835.
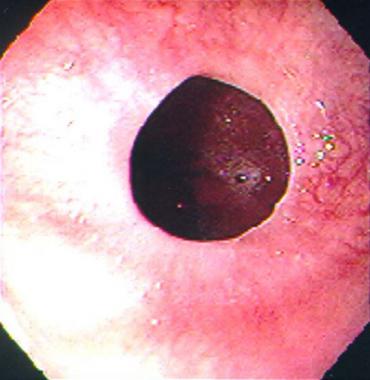
Podcast # 348: Steakhouse Syndrome
Author: Don Stader, MD Educational Pearls: Steakhouse syndrome is an impacted esophageal food bolus. Occurs because they have an esophageal stricture (schatzki ring, scarring, esophagitis). Classic treatments have consisted of effervescents, glucagon, and/or sublingual nitroglycerin (NTG). Recent case series has shown oral 400mcg tablet of NTG dissolved in 10cc tap water was 100% successful. Complications of NTG are hypotension and headache. References Kirchner GI, Zuber-Jerger I, Endlicher E, et al. (2011) Causes of bolus impaction in the esophagus. Surgical Endoscopy. 25:3170. Willenbring BA, et al. (2018). Oral Nitroglycerin Solution May Be Effective for Esophageal Food Impaction. Journal of Emergency Medicine. 54(5):678-680.

Podcast # 347: Fasting and Procedural Sedation
Author: Sam Killian, MD Educational Pearls: Recent study examining fasting and adverse events during procedural sedation found no association between fasting duration and any type of adverse event. Of the 6,183 children in the study, about 6 vomited during the procedure, and about 300 vomited recently after the procedure, and there were no episodes of aspiration. References Bhatt, M, et al. (2018). Association of Preprocedural Fasting With Outcomes of Emergency Department Sedation in Children. JAMA Pediatrics, doi: 10.1001/jamapediatrics.2018.0830. [Epub ahead of print]

Podcast # 346: Pediatric DKA
Author: Chris Holmes, MD Educational Pearls: There is a risk of cerebral edema in pediatrics with DKA if over resuscitated. Recent study comparing normal saline vs. ½ normal saline showed no difference in rates of cerebral edema regardless of rate of infusion. Recommend sticking with a fluid resuscitation protocol you are familiar with (i.e., 2 rounds of 10cc/kg bolus of NS). References Glaser, N. S., Ghetti, S., Casper, T. C., Dean, J. M., & Kuppermann, N. (2013). Pediatric Diabetic Ketoacidosis, Fluid Therapy and Cerebral Injury: The Design of a Factorial Randomized Controlled Trial. Pediatric Diabetes, 14(6), 435–446. http://doi.org/10.1111/pedi.12027

Podcast # 345: Epidural Abscess
Author: Sue Chilton, MD Educational Pearls: IV drug use and spinal procedures are major risk factors. Classic triad of back pain, focal neurological deficit and fever. However, presence of fever is highly variable. Neurologic deficits may not present until later, but then they can have a rapid progression of neurological decline. MRSA is most common organism, but GNR and MSSA are also possible. References Chen WC, Wang JL, Wang JT, et al. (2008). Spinal epidural abscess due to Staphylococcus aureus: clinical manifestations and outcomes. Journal of Microbiology, Immunology and Infection. 41:215. Danner RL, Hartman BJ. (1987).Update on spinal epidural abscess: 35 cases and review of the literature. Review of Infectious Disease. 9:265. Pfister H-W, Klein M, Tunkel AR, Scheld WM. Epidural abscess. In: Infections of the Central Nervous System, Fourth Edition, Scheld WM, Whitley RJ, Marra CM (Eds), Wolters Kluwer Health, Philadelphia 2014. p.550.

Podcast # 344: Foley troubleshooting
Author: Aaron Lessen, MD. Educational Pearls: When foley is stuck, balloon may not have deflated. Make sure balloon is not in the urethra, which can block drainage. Cut off the port as it may be obstructed. If still not draining, pass guide wire through port to unclog catheter. Other techniques have been described using mineral oil to dissolve, rupturing the balloon through over-inflation, and transcutaneous guided drainage. Crystallization can be a cause of catheter obstruction - sterile water may be a better solution to inflate the ballon than saline when it is first placed. References Khan SA, Landes F, Paola AS, Ferrarotto L. Emergency management of the nondeflating Foley catheter balloon. Am J Emerg Med. 1991 May;9(3):260-3. PubMed PMID: 2018599. Hollingsworth M, Quiroz F, Guralnick ML. The management of retained Foley catheters. Can J Urol. 2004 Feb;11(1):2163-6. PubMed PMID: 15003159.

Podcast # 343: Snake Bites
Educational Pearls: Snake bites commonly occur between April and October. Rattlesnake bites are the most common. Venom contains proteins/enzymes that cause local inflammation, coagulopathy, and systemic effects (hypotension, angioedema, renal failure, etc.) along with neurotoxins may cause fasciculations, ptosis, drooling, or hyporeflexia. Management: Mark site for swelling. Monitor progression. Elevate and immobilize injured limb and treat pain. Check basic labs including coagulation studies, and update tetanus. Antidote is CroFab and use if patient has systemic symptoms. Anaphylaxis is a known complication of CroFab Avoid: ice, tourniquets, and incision and drainage. References Hifumi T et. al.. Venomous snake bites: clinical diagnosis and treatment. J Intensive Care. 2015 Apr 1;3(1):16. doi: 10.1186/s40560-015-0081-8. Warrell DA. Snake bite. Lancet. 2010. 375(9708):77-88. doi: 10.1016/S0140-6736(09)61754-2. Warrell DA. Envenoming and injuries by venomous and nonvenomous reptiles worldwide. In: Wilderness Medicine, 6th Edition, Auerbach PS (Ed), Elsevier Mosby, Philadelphia 2012. p.1040.

Podcast # 342: Scombroid
Author: Jared Scott, MD Educational Pearls: Scombroid is a type of food poisoning associated with dark fish (i.e. tuna, salmon, mackerel) that mimics anaphylaxis. Occurs through conversion of histidine to histamine by bacteria in the fish. Symptoms include flushing, lips swelling, nausea, diarrhea in setting of recent fish consumption. Treat with antihistamines. References Ridolo E, Martignago I, Senna G, Ricci G. Scombroid syndrome: it seems to be fish allergy but... it isn't. Curr Opin Allergy Clin Immunol. 2016. 16(5):516-21. doi: 10.1097/ACI.0000000000000297. Patterson R, Little B, Tolan J, Sweeney C. How to manage a urinary catheter balloon that will not deflate. Int Urol Nephrol. 2006;38(1):57-61. Review. PubMed PMID: 16502053.
Podcast # 341: Tenecteplase vs. Alteplase
Author: Rachel Beham, PharmD Educational Pearls: Tenecteplase is more specific for fibrin and has a longer half-life than alteplase. In setting of ischemic stroke, tenecteplase before thrombectomy was associated with a statistically higher incidence of reperfusion and better functional outcome than alteplase. References Bruce C.V. Campbell B et al (2018). Tenecteplase versus Alteplase before Thrombectomy for Ischemic Stroke. New England Journal of Medicine. 378:1573-1582

Podcast # 340: Drowning
Author: Chris Holmes, MD Educational Pearls: Epidemiology: 80% male, ages 1-4 at greatest risk, African-American > Caucasian. Freshwater and ocean water may have more bacteria than pool water. Salt water is hyperosmolar, which theoretically increases risk of pulmonary edema. Greatest physiologic insult is from hypoxia secondary to fluid aspiration or laryngeal spasm. Patient survival is related to presentation on arrival. Workup includes CXR and ABG; consider C-spine immobilization/imaging when cervical injury is strongly suspected (i.e. diving injury). Treatment consists of supplemental oxygen therapy. Consider CPAP or intubation. References Szpilman D, Bierens JJ, Handley AJ, Orlowski JP. Drowning. N Engl J Med. 2012. 366(22):2102-10. doi: 10.1056/NEJMra1013317. Schmidt A, Sempsrott J. Drowning In The Adult Population: Emergency Department Resuscitation And Treatment. Emerg Med Pract. 2015. 17(5):1-18.

Podcast # 339: Ectopic Pregnancy Risk Factors
Author: Jared Scott, MD Educational Pearls: Data is mixed, but some studies show 1-2% of pregnancies are ectopic. Risk factors for ectopic pregnancies include: pelvic inflammatory disease, prior ectopic pregnancy, prior abdominal surgery, prior abortion, advanced maternal age, IUD, tubal blockage, and smoking (including spouse). Greatest risk factor is a prior ectopic pregnancy, which carries a 17x higher risk. Patients with histories of PID and cigarette smoking present educational opportunities. References Moini, A., Hosseini, R., Jahangiri, N., Shiva, M., & Akhoond, M. R. (2014). Risk factors for ectopic pregnancy: A case–control study. Journal of Research in Medical Sciences : The Official Journal of Isfahan University of Medical Sciences, 19(9), 844–849. Rana, P; Kazmi, I; Singh, R; Afzal, M; Al-Abbasi, FA; Aseeri, A; Singh, R; Khan, R; Anwar, F (2013). "Ectopic pregnancy: a review". Archives of Gynecology and Obstetrics. 288 (4): 747–57. doi: 10.1007/s00404-013-2929-2.

Podcast # 338: Mononucleosis predictors
Author: Chris Holmes, MD Educational Pearls: Symptoms commonly seen with mononucleosis are palatal petechiae, posterior cervical lymphadenopathy, inguinal/axillary lymphadenopathy, splenomegaly, and/or atypical lymphocytes > 10% on CBC. Among these, posterior cervical lymphadenopathy and atypical lymphocytes > 10% were the most sensitive (sensitivities of 0.64 and 0.66 respectively). References Welch, JL et al. What Elements Suggest Infectious Mononucleosis? Annals of Emergency Medicine. 2018. 71(4): 521-522. Doi: 10.1016/j.annemergmed.2017.06.014