
The Frontier Psychiatrists
102 episodes — Page 1 of 3
Getting our heads around the manosphere: two health professionals react
Introducing Brain Medicine
How To Ruin Your Relationships
One of the things I like about being on the Internet is that I get to meet the actual humans! There are people I've had real relationships with over many years, and some of them I've just never gotten to see in person yet. Making content on the Internet helps connect you to other people making content on the Internet, and if you're good at making friends, sometimes you can make a new friend. One such friend is featured in this podcast, and it's Annalisa Hanson—she is a therapist, who made some great content on TikTok, and then we hopped on the phone because we were such mutual fans, and then she joined me here on the podcast. Another guest on this episode is Dr. Mason Hargrave, we are also Clubhouse, and then he invited me to record a podcast in what was his apartment at the time. It's a classic.Today’s conversation grew out of a phone call with Annalisa and subsequent calls with Brandon In, Mason, Ahmed Tahseen, and my daughter Quinn.We “delve” into AI chatbots as a source of relationship advice. It’s quite the cautionary tale.The music is by Owen Muir, with some tunes a gift from my friend John Vanderslice. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Brain Stimulation (TMS) as a Treatment for Auditory Hallucinations
Schizophrenia is a really challenging illness. There's been a lot of progress made recently, I will note. I've already written about novel treatments like Cobenfy, and using accelerated transcranial magnetic stimulation for negative symptoms and positive symptoms in schizophrenia. One of the most bothersome of those “positive symptoms”—things that shouldn't be there, in someone's mind, but are—are auditory hallucinations. If you imagine having invisible AirPods that are playing a terrible podcast that you'd rather not be listening to, and that everyone else can't hear, you get a sense of how distracting it might be to have auditory hallucinations.In my previous article about the treatment of auditory hallucinations with transcranial magnetic stimulation (TMS), one of my favorite forms of brain stimulation, I highlighted promising results from early studies. Now we have a much larger Study, phase 3 trial, conducted over many years in Germany. We are even at the level of meta-analysis at this point!It’s a considerable study:138 adults with treatment-persistent auditory verbal hallucinations and schizophrenia spectrum disorder were randomly assigned (1:1) to receive 15 sessions of active (n=70) or sham cTBS (n=68) administered sequentially as 600 pulses to the left and 600 pulses to the right temporo-parietal cortex over a 3-week period.I called friends of the podcast—Dr. David Garrison, Dr. Will Sauve, and my mom, Vita Muir, to talk through this paper together, and what it might mean for individuals suffering from psychotic disorders. In the meantime, the team at Radial, where we provide such treatment, does some funny, tough-guy faces with our Ampa One system:Thanks for reading! A live-action newsletter event coming up on January 11th in San Francisco: RAMHT 2026 SF. Join us! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

A Breakthrough in Violence Prevention, by Treating Violent Criminals with MBT Therapy
I wrote an article about this research before, available here. However, I also made a podcast for my audience about the topic! Antisocial Personality Disorder is usually considered untreatable. A new study from the Anna Freud Centre’s MBT program demonstrates a remarkably effective treatment.At Radial, this is the modality of therapy we specialize in providing. It is also effective in borderline personality disorder and in suicidal adolescents. However, with some riffs, it turns out, it also helps ASPD. I even wrote a book on this a while back, published by Springer Nature (Amazon affiliate link).This conversation features my mom, Lila , and David Carreon, M.D..If you enjoy it, please share it with others! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Ep 98How I Wrote 966 Articles and 98 Podcasts in Three Years
This is the podcast version of yesterday’s article. Yes, I Know It Has A Different Title.Thanks for listening.And if you are looking for care for yourself or a loved one…join us at Radial—where I work—we focus on next-generation treatments.They include Spravato, Nightware, eTNS, PRISM Neurofeedback, soon, eCOT-AS by Neurolief, TMS, Accelerated TMS, and fMRI-guided SAINT TMS.Radial offers the most advanced mental health care, anywhere. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

How Can We Treat Bipolar Disorder in the Global South?
I was invited, thanks to the magnificent and only-ever-positive internet, to give a lecture to colleagues in Nigeria. I’m kidding, a little—the internet can be rough. Ask a comment section of a YouTube video! However, it is also a technology that has brought the world closer together. One of those less absurd corners of the internet is LinkedIn—it’s like the world’s most boring dad and his boss decided to invite you to a global-scale compliance educational module. “So exciting, it’s mandatory!”I am giving the internet a hard time. Sometimes it’s a special kind of magic. Like, for example, today. Imagine you are a progressive hospital system in Lagos, such as Gracehill Hospital. Yes, that is in Nigeria. It’s a progressive country, compared to the rest of the continent, but some of that progress is recent, as in 2023.A new Mental Health law was recently enacted in Nigeria to replace the Lunacy Ordinance of 1958. The passage of the new law was a major leap from the old. It was received with excitement because the former law was not only outdated but failed to address core issues such as the promotion of mental health and the protection of the rights of the mentally ill.If you're looking to move your healthcare system into the future, you might want to consider finding speakers for your grand rounds. With Zoom, it’s easy to host hundreds of people. On LinkedIn, you can see professionals posting about what they are up to. And, if you're bold, you can simply ask one of those folks to speak. Which is what happened to me, and how I found myself drafting a lecture on Bipolar Disorder for an audience of Nigerian (and global—many people, both professionals, patients, and family members attend these seminars!).Nigeria has an estimated 250 practicing psychiatrists for a population of over 220 million (WHO, 2023), amounting to roughly one psychiatrist per 880,000 people. I probably spoke to 1/4 of them yesterday.There are substantial barriers to mental health care in Nigeria—much if it financial. According to the World Bank, Nigeria’s Gross National Income (GNI) per capita in 2023 was $2,460 USD. Fewer than 10% of Nigerians have health insurance. Those plans cost $250+ a year, but mental health parity doesn’t exist, and thus those services are only covered under yet more expensive plans.To draw a direct comparison, Nigeria has 0.11 psychiatrists /100,000 population. This is similar to Kenya (0.2/100,000) but with 400% more money budgeted to address the care of the population. The US has 13/100,000 and spends about 6.2% of its health budget on mental health care.The question, globally, is how to do more for our patients with less harm and at lower cost. One interventional treatment is considered essential—and its ECT. The WHO's keep an “essential medicines” list! Nigeria has access to ECT. Lithium is also an essential medicine. TMS is not on that list, yet. Maybe, I posit, it should be?What follows in this podcast is the talk I gave. Thanks for reading— and listening. A huge shout out to my gracious hosts at GraceHill, and their Partners, who make this series possible!The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.If you are interested in the Validation Institute’s award for Best Mental Health Treatment in 2024, consider Radial. It’s where I work, and with locations across the US already, we are working to bring the most advanced mental health care to everyone and make it accessible. If you are looking for help, Radial offers the most advanced mental health care. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Ketamine in the Land of Taylor Swift
One of my great joys as a psychiatrist is the ability to collaborate with excellent colleagues. Irfan Handoo, M.D., of Kansas City Psychiatric Partners, is one such human. In this interview, we learn about how Dr. Handoo went from psychopharmacologist to interventional psychiatrist, why Kansas City is the best city in the world, and why being South Asian is the ultimate hack to get your patients the best care. It's really easy to think of doctors being completely burned out, and not caring about their patients. Being a physician is a tremendously challenging thing to do with one’s time, and many doctors have their compassion wear thin. This interview with Dr Handoo reminded me how much some of us care, all day, every day. He's an inspiration to me, and I hope, to my listeners also.I am delighted to bring you this interview! Prior articles featuring the work of Dr. Handoo include:Thanks for reading and listening!The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Suicide Among Resident Physicians
Every once in a while, science authors will crank out a paper that answers some questions, but asks so many more. I’ve been talking, writing, and podcasting about physician suicide longer than most other topics in my creative life.I did a whole award-winning series as a Rudin Master Scholar in Ethics and Humanities, which no one noticed. Including podcasts like these:and this…and this…Today’s podcast is instead of a written column. Feel free to listen. The paper it’s about is here:Causes of Death Among US Medical ResidentsIt was published on May 14, 2025. Please read it, listen to the podcast, and share with your world. It’s a challenging path, that of physicians, and we should consider making it less miserable, for all our sakes. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Say His Name: Five Years Since Mr. George Floyd
Author’s Note: This writing was adapted from a series of conversations around race in America and edited as audio, recorded in 2020, right after George Floyd was lynched.. The podcast of this writing is the real thing, as it were. What follows is edited text to clarify the narrators, absent the audio. Please consider following the podcast associated with this newsletter and leaving a 5-star review on Spotify or Apple Podcasts. Please subscribe to support high-impact content like this.The author, David Foster Wallace, described the experience of reading his novel Infinite Jest as intended to feel “tornadic,” like you're in the middle of a tornado. That's what the last several weeks have felt like.Protesters:"Racist ass police! No justice, no peace! F**k these racist ass police! No justice, no peace!""F**k these racist ass police!"Owen Muir, M.D.:I originally tried making this episode a linear narrative, but it wasn't happening. So, welcome to the tornado of racism in America. Buckle up.George Floyd spent 8 minutes and 46 seconds gasping for breath. Police officers, some of whom were very experienced, knelt on his back...until he didn't breathe anymore. As a psychiatrist, I often emphasize how the words we use to describe someone's death have meaning. So, I'll say, you know, completed suicide, not “commit.” And George Floyd was lynched.Welcome. This is about anxiety, uncertainty, and existential despair. And I recorded the narration in one take because I wasn't, like, going to get it right a second time. So much of what we say about race is calculated, polite, and wrong. So I'm not going to try to do that tonight.Here we go.Sequoiah:"Yeah. My general reaction to all this is a little more, a little more extended. The, uh, f**k".Owen Muir, M.D.:That's my teammate. She is a TMS technician at the mental health practice we worked at together. She also works in the community with patients helping put their lives together, but tonight she's a field reporter on the revolution.Sequoiah:"I am a TMS tech, Winnicott coach, and black woman. Which seems very important right now. George Floyd, Say His Name. George Floyd, Say his Name.So I just got home from a protest in Flatbush. Police would not let us pass. We were chanting with our hands up. And after a while, they decided to push the line backward. We resisted—we stood there with our hands up. They pushed us and pushed us, and when we wouldn't..."Owen:Now, as someone with a lot of white privilege, I'm outraged at hearing this, like, wow, this is fucked up. So I called another colleague in the special operations community, and I'm not using names in this episode for semi-obvious reasons, and I heard what he had to say.Master Sergeant:“The things that U. S. police forces are apparently fully within their legal rights to do, like, use tear gas, would literally have…been against the Geneva Conventions. It's an actual war crime. We cannot gas a civilian population.”Owen Muir, M.D.:The person I’m interviewing has over a decade of experience in the special operations community. He has fought and killed for our right to do what my other colleagues were in the street doing, peacefully protesting.Master Sergeant:"This is a perversion of what the United States stands for. We invade countries who treat their people the way that our police forces are on camera treating Americans "Sequoiah:"People started to back up, , and run and they then started to hit us with batons. , I fell. And then we reformed the line."Master Sergeant:"It's disgusting in a lot of ways."Owen Muir, M.D.:So when someone whose life has been dedicated to protecting our freedoms tells me they're upset with what they're seeing, I take that pretty seriously.Sequoiah:"Well, the other night, well, last night, when the cops and protestors were getting into, into fights and they were trying to, the cops were trying to push back the protestors, I saw them bring out the batons and, like, start attacking people...and each time they'd tell us to back up and back up and kept pushing us and pushing us. And finally, there was a frustration in the air, and people started to act out."Owen Muir, M.D.:Now, as a psychiatrist, my life has been saved by police officers on more than one occasion. I have been physically attacked in hospital settings. The police have been called, and I have not died, and my colleagues have not died thanks to them. And this is Flatbush, Brooklyn, New York, and these people are black people. The Flatbush, at least the area I was in, is a predominantly black neighborhood. So, look, Americans love the police. They are a highly regarded part of society by many people, but that's not the experience for black America I have learned.Master Sergeant:“There are many things you can do in that spectrum that don't involve actively using force against a human being, which makes the process easier across the board. If I don't have to hurt somebody, the only thing that is hurting another person does for me is further e

The Scalable Depression Solution
Owen Muir, M.D. of The Frontier P This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Tardive Dyskinesia: Do I Have It?
Oh my. The irony is thick with this one. Your author, and sometimes scientist, Owen Scott Muir, M.D. has been doing research on Tardive Dyskinesia. And…he might have the disorder. The search function lets you search for other articles on the topic. If you are interested in treatments for psychiatric disorders that don't cause this adverse effect—a permanent movement disorder—they exist. The care we provide in New York, California, and now, South Carolina works, diligently, to advance the science of safer treatment. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Can Inflammation Status Predict Response to Depression Treatment?
The frontier Psychiatrists breaks down a publication on the topic of immune modulation of TMS response in depression. And Dr. Owen Muir explains what inflammation is for mental health conditions in the process. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Plague Of Athens Podcast
I’ve been obsessed with the Peloponnesian War as a historical event for 20 years now. I wrote an article about it recently, and also recorded a song about it many years back.Enjoy the listen!If you like the music, there is more of it on Spotify…The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

S2 Ep 1How Did Rapid Remission from Depression Become the New Standard of Care?
This podcast was edited on a plane ride to Japan, and the intro was recorded in a bathroom while my kids slept off the jet lag. It’s still good. I recently went down with Ben Greenzweig, the Executive Director of the non-profit Living Water Brain Treatment Center in Myrtle Beach, South Carolina. We are—right now—providing TMS treatment and, soon to be more, in a local community in Ben’s beloved home of Horry County. There are 400,000 residents and less than 30 psychiatric inpatient beds in the county. There are not enough services to meet the needs he saw in his community—so he started Living Water to help. I’ll remind readers that not only did he write an article about it, but he is also running a non-profit. Thus, consider donating.The audio from today’s podcast was recorded mainly on my phone, which I had in my pocket as I gave the talk. Please share it with friends. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Mystery of Machine Gun Kelly
My readers and listeners know that this project, The Frontier Psychiatrists, is daily. Sometimes, I don't get the thing done till the end of the day. Today is one of those days. I was running on empty when it came to narrative this morning, so I decided to try to make a podcast. One of the tricky things about these more experimental days is that I don't know if the story is going to work. It's like walking a tightrope. I'll choose something— anything— to write about. And today I decide to make it even more difficult for myself, because I didn't feel like typing anything, and so I made a podcast instead. Today's was going to be about Machine Gun Kelly and being old. That's all I knew. The podcast you're about to listen to explains what happened, and the lessons I took away from the journey of trying to figure out who the heck Machine Gun Kelly is. The podcast features some of my favorite people, including Michelle Bernabe, RN , Courtny Hopen, RN, and my mom, Vita Muir. Surprisingly, it ends up featuring Drew Barrymore, and I'll let you listen to figure out how that happened. Thanks for joining me on this publication's experimental journey. I really hope you listen to the episode. It took all day to land, and I think it's good enough.Yes, the podcast was created—top to bottom— today. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
Why Ketamine Clinics Keep Closing
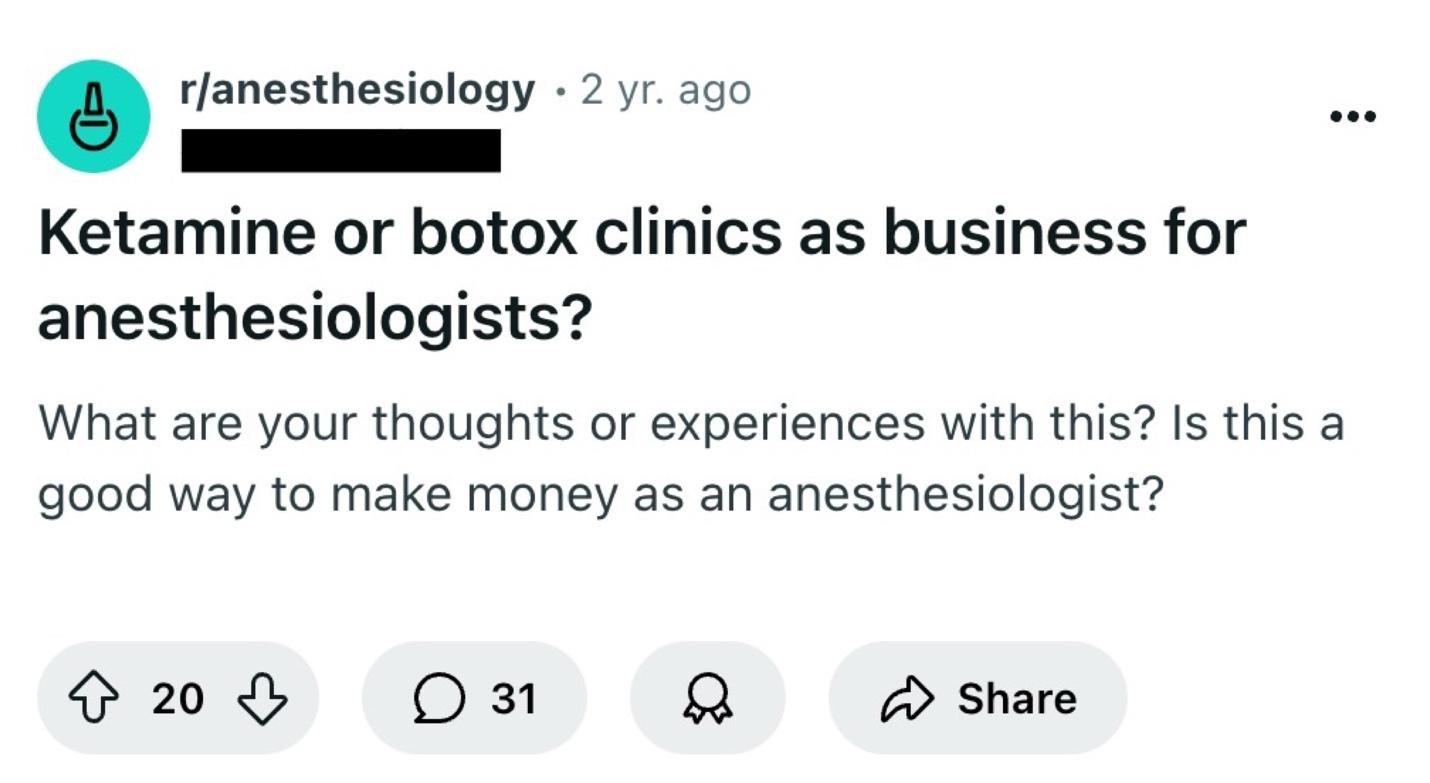
Today, The Frontier Psychatrists welcomes back my friend Ben Spielberg. He's been a reader for a long time and has contributed to the newsletter in the past. It was on Clinical Trial design, a perennial favorite around these parts.With only light edits, what follows is his work, narrated by me, for the Audio Version.I would invite you to the live class today on working as an out-of-network provider, but it sold out last night, so you'll have to wait for the next one. My prior article on Spravato is available here.The year is 2024. OpenAI has just launched its latest update to ChatGPT, promising more natural and less artificial-sounding language. Donald Trump has won the nomination for President of the United States. Another chain of ketamine clinics has engaged in a corporate reorganization. There is conflict in the Middle East. Are we sure that we're not living Groundhog's Day?I am the founder of Bespoke Treatment, an integrative mental health facility with multiple locations that has at times been referred to as a "ketamine clinic." I have also seen countless so-called "ketamine clinics" sell for pennies on the dollar and go bankrupt seemingly overnight. In this case, Numinus, a company that was publicly traded in Canada and owned a number of psychiatric clinics specializing in ketamine in the US and Canada, has sold its clinics to Stella (a company that has stealthily become one of the larger mental health providers in the country and is the first to bring the awesome SGB treatment to scale). It's not the first time this has happened. It's not the second, nor the third, nor even the fourth time this has happened. But yet, the common consensus is that ketamine clinics are a cheap, easy business with recurring revenue. So, what gives?Figure 1. A reddit user asking anesthesiologists if they should start a ketamine or Botox clinic for easy cash on the side. Does this make you feel gross? Should it?The Ketamine Clinic Model 101The most basic outline for a ketamine clinic is as follows: a provider rents an office space with, on average, five or so exam rooms. They buy equipment for infusions like a pump, catheter, needles, and syringes. They buy some comfortable recliner chairs. They hire a receptionist to answer phones, field patient questions, charge credit cards, and handle medical record requests. They hire a nurse to insert the IV, monitor vital signs, check blood pressure, juggle multiple patients at once, and make sure the ketamine is flowing into patients’ veins unencumbered. Two SKUs are typically offered: ketamine infusions for mood, which last approximately 40 minutes, and ketamine infusions for pain, which last for up to 4 hours. Zofran is offered for nausea, and some clinics have fun add-ons like magnesium or NAD. An average mood infusion costs around $400-$500 in a medium cost-of-living area, while mood-infusions can run up to $700 in a higher cost-of-living area. Some clinics offer package discounts if patients buy six or more upfront, which helps with cash flow for the clinic (cash now is better than cash later, of course).A Note on Scope of PracticeThe first wave of ketamine clinics was started mainly by providers who were not mental health specialists. Instead, they were owned by anesthesiologists, ER physicians, and sometimes CRNAs. These providers were especially experienced with ketamine in hospital settings, as well as setting up infusions. Psychiatrists, on the other hand, do not usually order infusions in outpatient settings, and very few had actual hands-on experience with ketamine in practice. That being said, there are a number of variations to the model above: psychiatrist-owned ketamine clinics would often prefer to use intramuscular injections in lieu of infusions, but 2-3 injections would have to be given during a single session for mood and pain sessions were out of the question. Other ways to save costs might include having an EMT do the actual injections (this is highly state-dependent), asking nurses or MAs to work the front desk, or working a full-time regular doctor job. In contrast, your nurses run the actual ketamine services via standing orders, a written document that details routine and emergent instructions for the clinic.Some clinics offer full evaluations prior to rendering treatment, but many offer a simple brief screening on the phone to check for contraindications before scheduling a patient for their first session. The clinics owned by psychiatrists have historically been a bit more thorough in terms of the initial psychiatric evaluations, given that they can actually perform initial psychiatric evaluations within their respective scope of practice. Sometimes clinics may have therapists on-site who can render ketamine assisted therapy (meaning, therapy occurring concurrently) for an additional $100-$300. Otherwise, there is not much decision-making that goes on— other than deciding on medication dosages. Most infusions start off at .5mg/kg of body weight, which

Building Trust In Clinical Trials
The Frontier Psychiatrists is a daily-enough health-themed publication. But sometimes, I just want to make a podcast. Today is one such day.Enjoy!The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

THIS IS NOT THE WAY: CEO of UnitedHealthcare Murdered in Midtown Manhattan
Today is a day of mourning. In broad daylight, in the city I love, Brian Thompson, the CEO of UnitedHealthcare’s insurance subsidiary, was murdered. According to CNN:Brian Thompson was walking toward the New York Hilton Hotel in Midtown Manhattan, dressed in a suit and tie, to attend UnitedHealthcare’s annual investor conference being held in the ballroom.A gunman, who investigators tell CNN was masked in the sub-freezing temperatures, waited for about 10 minutes before Thompson’s arrival, before opening fire from 20 feet away shooting multiple times, striking Thompson.The gunman fled, cutting through an alleyway and hopping on to a bicycle, the official told CNN. Investigators are continuing to canvas the area. Police currently believe that the suspect fled into Central Park.Brian was 50 years old. I don't know the man, personally. I do know that he was doing his job, and somebody murdered him in cold blood.This is not the way. Assassinations are not how we resolve disputes in a civil society. I get frustrated with United Healthcare, and I make fun of them for some of their decisions. This should never be mistaken for malice: these people are doing their jobs, just like the rest of us. They need to feel safe to make good decisions. They deserve to feel safe, even if they make what some might consider bad decisions. There is no level of a bad decision in a business context that gives anybody the right to put a bullet in your chest.I don't know why this masked shooter did it; I'm guessing this was somebody with a rationale of their own. We'll find out—or we won’t. But none of us should celebrate this; everyone should decry targeted violence.It's also worth noting that United Healthcare's decisions have made people tremendously angry. Your anger about a business policy isn’t an excuse to joke about someone’s murder. This is a man with a family, friends, and loved ones.This isn’t remotely funny. This isn’t ok. Mr. Thompson and all of us deserved better.Let’s all get on our knees and pray that this sort of violence leaves our cities and threatens our lives no more. We can have disputes about best practices and employment law like adults, but never, ever should we make light of the murder of a man who deserved dignity and life.Today, I stand unapologetically and without hesitation with UnitedHealthcare and its team. You are loved and deserve better. I hope and pray for justice and healing. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

RFK (the) II Tries Out For Richard (the) III
Synopsis:Bobby, alone on the side of the road driving back to Manhattan after loading a bear carcass into his Cybertruck, reveals his intention to play the villain. He then pretends to console Donald, the first victim of this villainy. After Donald is led off toward the White House, Bobby greets Elon, who tells him that someone is very ill from an infectious disease. Bobby, once again alone onstage, outlines his plan to have Donald killed by preventable illness and to marry Lady Melania.—Act I, Scene IBobby: Now is the administration of our discontent Made glorious summer by this son of New York Real Estate, And all the regulatory burdens that loured upon our agency, In the deep bottom of the grave, buried. Now are our Houses of Congress o’erflowing with victorious representatives, Our primary battles ceased, and our districts justly called, Our stern alarums about “voter fraud” turned to merry winnings, Our dreadful attack ads to smug tweets. Grim-messaged campaigns hath chilled the f- out; And now, instead of threatening election workers with a bloody revolution To fright the souls of LibTards, Donald Capers clumsily in Laura Loomer’s chamber, But I, who am well-shaped for sportive adventures thanks to my healthy diet, And made to drink raw milk from a cool glass; I, that am built, healthy, robust, and also sexually functional To strut before a wanton ambling nymph such as Melania; I, that am curtailed of his fair proportion of the wives of others, Cheated of affairs by regulatory limits on supplements to enhance my male nature, Unengorged, under aroused, sent before my tumescence Into this bedroom scarce half ready, And that so lamely and lacking prompt virility That ladies will ask, “Are you ready?” and “Maybe this is a bad time?” as I prepare for them — Why, I, in this weak piping time of GOP dominance, Have no delight to pass away the time, Unless to see my manly shadow in the sun And be impressed by my physique. And therefore, since I cannot prove a lover To entertain these fair, well-spoken days, I am determined to prove a villain, and hate the regulations that might limit my consumption of supplements and medicines to enhance the idle pleasures of these days. Plots have I laid, regulations dangerous, By drunken prophecies, libels, and appointments to agencies that I have no business running, To set my friend Donald and Elon In deadly hate, the one against the other; And if Elon be as Bold and Ambitious As I am subtle, false, and treacherous, This day, should Donald be held up About an Infowars story, reposted on Breitbart and OAN, that says that “RFK” Of JFK’s heirs, the most important appointment, shall be. Dive, thoughts, down to my soul. Here Donald Comes! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
Cobenfy
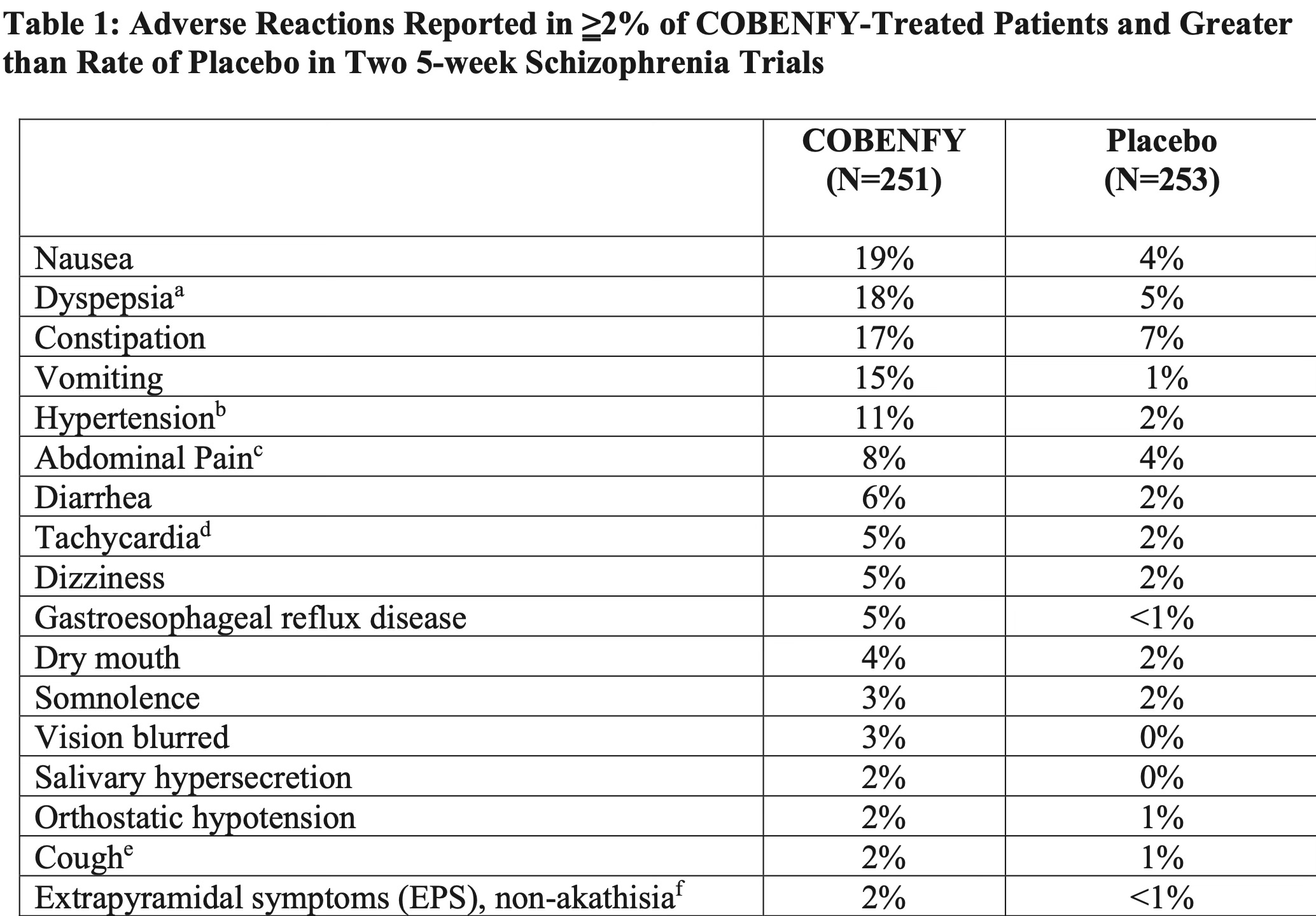
The path from xanomeline to the brand name treatment named Cobenfy was a long one. Cobenfy is FDA-approved for the treatment of Schizophrenia. Here is the literal label:COBENFY is a combination of xanomeline, a muscarinic agonist, and trospium chloride, a muscarinic antagonist, indicated for the treatment of schizophrenia in adults.To people who haven't yet read my book Inessential Pharmacology, (Amazon Affiliate Link), I will highlight that this is approved as a monotherapy. That means it can be prescribed as the only drug for people with Schizophrenia.It has a completely different mechanism from every other antipsychotic. All the others block or modulate dopamine to some degree. Those are the variety of drugs I have written about, in less than glowing terms, in some cases.These are medicines that lead to obesity and early death (particularly in youth on Medicaid). I have argued they should never be used as augmentation agents.I argue, in fairness, a lot of things. One of the things I have argued about regularly is that individuals, particularly those suffering from devastating illnesses like schizophrenia, deserve treatment that works. That same treatment best if it doesn't harm the person also. The problem with antipsychotic medication is that they regularly harm the people who take them.Finally, we have a new drug that is helpful for individuals with schizophrenia and less harmful in terms of catastrophic adverse events like massive weight gain and tardive dyskinesia.What are the adverse effects for Cobenfy? Yes, those used to be called side effects.It's overwhelmingly causing problems related to nausea or other predictable anticholinergic side effects in the peripheral nervous system, especially the G.I. tract. I'm not saying it doesn't suck. I'm not saying it doesn't have side effects. But what you don't see there is massive weight gain. What you don't see there is permanent movement disorders. Does it work? In short, yes, it works. Nothing works fabulously well in schizophrenia yet, but it's not a slouch treatment, and it's not worse than existing drugs at least in the people they already studied (again, from their submission to the FDA):It's the first not me-too for schizophrenia, since clozapine. It's got a restricted range of side effects that are annoying, but not life-threatening. Will we discover more at large scale? Probably.Bristol Meyers Squibb is not done yet. They are going to be bringing this drug to bipolar disorder, and other conditions. Let's reduce the risk of early death from dopamine blocking medications for everyone for whom that would be beneficial.I'm at a conference, so I'll keep this one concise, because I'm writing it on my phone. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Doctors of Scale
I was at AACAP and sat down with Dr. Sood, a colleague, and we had a chat about investing, goal setting, venture scaleable businesses, and private equity, and we had some fun at the expense of Red Lobster in the process. I hope my colleagues enjoy the listen!Prior articles on the topic include What If We Didn’t Blow The Horn, Private Equity Sucks at Running Business of Medicine, and more. Thanks for reading and listening, and Ashwin for joining me! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Culture of Burnout
This Podcast is a recording of departmental grand rounds presented at the Medical University of South Alabama pre-pandemic on burnout. It references a long legal back and forth I’d put up with. That has led to, last year, our legal team filing a defamation lawsuit and, this week, a request for an injunction. It’s more burnout than when I did the talk. I hope it’s still a source of sassy wisdom about what physicians must do to keep their heads in the game, care for patients, and respond with sense and compassion. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Why Bipolar Depression Gets Worse In The Fall with Dr. Owen Muir, M.D.
The Frontier Psychiatrists is a daily health-themed newsletter. My dear friend Courtny —who recently penned an awesome guest post— reminded me that Fall is here. And with it, seasonal changes in mood for those with Bipolar Disorder. I’ve written about having bipolar disorder before, in a letter to that disorder. I’ve written about how important sleep is to not die. I’ve even written about this specific topic—circadian rhythm changes in bipolar illness, in a prior article here. But who has the time to read anymore? Isn’t there a video or podcast I can view without having to read all those linked articles? Yes, now there is. It’s here, now, for you, my dear subscribers. I’ve got music on Spotify! I even have a book on Amazon…(affiliate link). Oh, and another book of poetry. And a therapy manual. Thanks for reading, viewing, and listening. Oh, and…50% of subscriptions to help you cope with depressing changes in lighting. A special discount is available to celebrate fall by clicking here!The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Infidelity: A Failure of Mentalizing?
This newsletter is quite the multi-media shop. It gave me a new tool here on Substack, and I’ll use it less-than-polishedly. I wrote a column earlier this week on infidelity, which seemed to strike a chord. This video experiment was created in response to reader feedback on that piece of writing. It’s a new format for me and far from perfect. Let me know if you dig it anyway.Remember—I’ve got music on Spotify!I’m broadly not very talented in a wide range of media.The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Everything You Ever Wanted Broke My Heart
My mom and dad left a lot unsaid between them, and after his second stroke, the ability to have the conversation that they had put off? It was like visiting a ski slope in the summer. You can see the runs, you can see where the snow would have been, and imagine the speed, the presence, the thrill, breath taking cold. But none of it is that, at that moment. Many close relationships are actually three relationships happening at once. One relationship is the explicit relationship— what you say to each other. The others live inside each of your heads, separately, and it's all the things you haven't said. Explicit is shared, and the implicit are islands, in the middle of the Pacific, surrounded by saltwater, perilous to approach. Only the most intrepid ever approach these islands of the inside and the unsaid.It remains to be seen why what we don't say is so scary. Maybe it's the sharks we imagine in the water? Maybe it's the dying of thirst on the way there? Maybe once you get there, you wouldn't like what you found? Maybe you will kill everyone who lives in that island with the memetic infections, vector-borne diseases of the explicit?A plague, that's what you didn't talk about…maybe. Some of us have a different set of experiences, are novelty seeking, and will take a risk. Some of us have already drowned once, and been revived.There's a secret, it turns out, to finding everything you ever wanted, across expenses, time, Atlantics away. There's a way to traverse the gap between each other. It requires understanding that you don't understand anybody else. It starts by acknowledging that you haven't said the most important things—and neither has he, she, they. The same fear that drives you drives everybody else, to an uncomfortable small talk, instead of impossible silence, with all the weight of all the things that you were afraid to say. I love you, and worse, I loved you. Past-tense, tense. I hated you, once. I did things I regret. I fear things that you have left, in another life, on another continent, frozen deep in the ice of the Antarctic, and boiling away in the water around that volcano. In letting our fears guide our conversations, and their malicious edits, we leave each other bereft—the walking dead.The truth is we're gonna die, together or apart, and living together, with the most important things kept unsaid is as pointless as it is poisonous.All of us have something to own up to. The sooner we do it, the less lonely and dead we are.In Memoriam, Jake Seliger.If you don't read Bess Stillman, now is the time. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
Don't Lie to Congress: Advice to the Leadership of Pharmacy Benefit Managers
Recently, the leadership of all three big health PBMs testified in front of Congress…and…have now been asked to correct the congressional record.So, I made a podcast instead of an article about it today cause my kids are away, and I love the format. I hope you all enjoy it. The transcript is in the top right if you just want to read, and not listen!A few prior articles include:The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Wizard Of Odds, Ch 1
The Frontier Psychiatrists is a daily enough health-themed publication. It’s also a podcast. Sometimes, I need a break from serious coverage of policy. In those cases, I amuse myself with David Foster Wallace-esque fan fiction about health policy, like this first chapter in my Wizard of Oz-themed parody about health insurance. Dorothy gets strep…then psoriasis…then OCD! Join us for a little health-themed absurdity, and maybe, just maybe, we will all learn something.The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

PRISM: Trauma Treatment You Don't Need to Talk About
I have been writing about PTSD treatments quite a bit in The Frontier Psychiatrists newsletter. One is offered at Fermata, the clinic I co-run in Brooklyn. I recently wrote an article about it. We provide Prism treatment for PTSD at our clinic, much like our colleagues at Homebase in Boston, with Veteran Populations.Sometimes, you’d rather listen. On that note, here is the podcast version of that article.Other PTSD-themed writing includes…Medical Cannabis for PTSD?PrazosinThe ICU is Traumatic For EveryoneAs well as a whole… Saga… on MDMA:Can MDMA-AT Be Saved, Part ICan MDMA-AT Be Saved, Part IIShould MDMA-AT Be Saved, Part IIISaving MDMA from AT: Part IVBad Touch!: MDMA Part VSaving MDMA (and other psychedelic therapies), Part VISaving MDMA VII: This Isn't The First Drug to Have Problems Getting ApprovedIt’s worth noting I’ll be appearing on a webinar with the Psychedelic Medicine Association to discuss the following…and I’ll include the info from my friend and co-author Dr. Morski, MD, JD:The FDA Said No, What’s Next? Exploring the Field’s Next Chapter After the MDMA DecisionRegister now!In case you missed the news last week, the FDA officially denied Lykos Therapeutics’ New Drug Application for MDMA-assisted therapy, requesting a new Phase III trial be conducted. This was a huge blow to the practitioners and patients who were hoping that MDMA would soon be a legal option to address PTSD, a condition where no other therapy has shown the same levels of efficacy as MDMA-assisted therapy.So you may have questions, like, “When is the next psychedelic medicine likely to be up for FDA approval” and “Which medicine may be the next to reach that stage?” And you may also want an update on what psychedelics (like ketamine) are legally available and how might they serve as a stand-in for the others while we await FDA approvals.This month we are truly fortunate to have panelists working in various arenas within psychedelic medicine and research to help lead a discussion regarding what psychedelic options are currently available and what’s to come, including:* Which psychedelic medicines are next in the FDA pipeline* When might we see another psychedelic therapy up for FDA approval* How can we utilize the available psychedelic options in the meantime...and much more!Register now!Panelists joining us for this month's event are:* Owen Muir, MD, DFAACAP | Co-Founder, Fermata; Chief Medical Officer, iRxReminder* Carlene MacMillan, MD, FCTMSS, DFAACAP | Co-Founder, Fermata; Chief Medical Officer, OsmindYou can learn more about them on our event page.So please join us for this live panel discussion on Thursday, August 29th at 5 pm Pacific, 8 pm Eastern. A link to the recording will be provided afterward if you cannot make it to the live event.Hope to see you all on the 29th!You can find the Psychedelic Medicine Association on Twitter , LinkedIn, and Facebook.In service,Lynn Marie Morski, MD, JDPresident, Psychedelic Medicine Association This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
Open Comment Outsiders
My friend and RAMHT co-founder, Grady Hannah, had a quick and dirty conversation with two friends today about the thrilling 2025 CMS Physician Fee Schedule. Every year, there is an open comment period on these proposed changes, and this year has some crucial changes for physicians who’d love to be able to deploy Digital Theraputics in the context of Behavioral Health Disorders.Thanks for listening. More coverage of this open comment period is coming soon, but here is a quick overview of the issues at stake. Yes, this is how nerdy we are at baseline. Yes, we talk like this to each other for fun. This time, we recorded it. Yes, I am this boring. Thank you so much for listening! As a reminder, I have a new book out, and it is available on the Kindle store! It’s the number one new release in:DepressionPharmacologyHumor: Doctors and MedicineAnd it’s inching up to #11 on the “just generally funny books” charts. Let’s push this one to number one among all funny-ish books.It’s called Inessential Pharmacology. (amazon link) This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
Warning Labels For Social Media Are A Terrible Idea...A Podcast with Owen Muir, M.D.
Yesterday’s column was a fine article, but what if you miss my snarky tone while reading it to yourself? Problem? Solved. Dear Readers, here is the podcast version of the aforementioned article!For those hoping for actual solutions? The AACAP Facts for Families series of guides exist! For example, you can learn how to prepare for your child’s first cell phone. You can also get expert guidance from actual child psychiatry doctors on Internet Use In Children. Or we could follow scaremongering from the Surgeon General? That is also an option.My ChatGPT prompt: “Please generate a scary warning label for social media that the surgeon general could place on social media platforms that would terrify young people into not using social media quite as much.”Here is the warning label it came up with:I think we are really getting somewhere. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

We Need to Talk About Mental Health*
The Frontier Psychiatrists started as a room in on the clubhouse app. One of the enduring pleasures from that era is my friendship with @Psych Fox (Jeremy Fox, P.C.). He’s a licensed professional counselor, EMDR therapist, and a delight to speak with. This week’s podcast features a discussion of a paper Jeremy brought to the table:Are mental health awareness efforts contributing to the rise in reported mental health problems? A call to test the prevalence inflation hypothesisThe inflation hypothesis posits that more talking about mental health problems leads to more actual problems. We also discuss the role of screening, including my very popular thoughts on the DSM-5-TR Level One Cross-Cutting Measure, as featured in my Osmind EHR, that I use in my work at Fermata.In our conversation, we evaluated the possible takes on this paper. While I’m at it, I’ll remind readers that suicide risk assessment is important, and no one does a better job of explaining it than Dr. Tyler Black:Thank you for listening! Please share this podcast with your friends drop a a 5-star review on Apple Podcasts. It drives discovery like woah. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Accelerated Transcranial Magnetic Stimulation (aTMS), Explained
The Frontier Psychiatrists newsletter and podcast do a lot of cheerleading for brain stimulation—particularly accelerated TMS. However, I’ve recently added many new readers and have not explained my favorite brain stimulation approach. The podcast version and a useful transcript are intended for educational value. Also, here is Garfield:Prior articles on the topic are myriad, but include:This comprehensive explainer all about accelerated TMS over at the Radial blog. TMS is better than DrugsTMS Should be Covered by Medicaid Depression Can Be Over in 5 Days, ReplicatedThe Science Behind the Best Outcomes In Mental HealthYour Depression Should Be Over AlreadyMy Sickboy Podcast AppearanceAnd many others!Thanks for reading, listening, and sharing. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Mental Health Crisis
The following is a brief explanation of an overarching point of this newsletter: The Frontier Psychiatrists, for new and old readers alike.It's mostly penned, in the Apple Pencil Pro sense of the word, by Owen Scott Muir, M.D., although I sometimes have guests. We already have a diffusion product: the series of RAMHT events! That's “rapid-acting mental health treatment,” co-created with Grady Hannah.A crisis is not just a problem. It’s not just problems—plural. It’s the admixture of problems with hopelessness. This newsletter is written to go beyond providing “solutions to problems.” We have those already. If we knew we had problems with solutions at the ready? That does not meet “crisis criteria.” We need to address the crisis mentality surrounding the difficulties we face in our minds. Panic is sometimes understandable in that it can mobilize life-protecting responses in the context of imminent death by, for example, tiger maw. However, panic is axiomatically not rational. In a crisis that involves solutions that extend to payment models, policy, and complex systems? It becomes a truism that demonstrably neither panic nor crisis mentality will do anything useful.We do not have a mental health crisis. We have a mental health crisis…crisis. We have become so panicked by the relentless onslaught of early, preventable death, loss, and sorrow that we cannot address it. The crisis frame creates panicked responses. Those responses have served up more death, suffering, and isolation.No thanks, I say. This newsletter is written to address the “mental health crisis” as something other than a crisis. We face understandable problems with rational solutions—if we can think clearly. Some of what I have written is funny. It might be gallows humor. It might be absurdist. This serves two purposes—one, it is hard to laugh and panic at the same time. The message is the medicine. The second is more self-serving. I just can’t stand writing the number of words that will be necessary without having some fun, personally. I wish I could. I can’t. Other people write deeply serious tracts. Read those, if this is no laughing matter.In my attempt to dismantle the crisis mentality, I am not stopping at one word. I’m going after the whole phrase. I’m a serial killer for “the mental health crisis.” Only the article—“The”—will be left standing by the end.People use the term “mental health” more often than they mean it—by a factor of always. One of my favorite pandemic-era malapropisms-in-waiting is the saying: “Everyone has mental health.” What I imagine people mean to say, with the stigma baked right in, is that everyone has some degree of psychopathology. Everyone has problems. Does everyone have a risk for mental illness? Everyone has a mental state—it’s glib. It is maximally-pointless pablum.Mental health is a nonsense phrase, and I will dispense with it as useful. Mental Health is a state of health as it applies to the mind. Perhaps there is an absence of problems with the brain, mind, and spirit? It’s as meaningful as saying, “Everyone has bones” at an orthopedic professional society meeting. The presence of bones are not at issue for orthopedics. It’s the fractures of said bones that matter. “Everyone is a little bit crazy” is the kind of thing generally well people can say. This is in the same way that other generally well people can claim there is no such thing as a psychiatric illness. Both statements are inaccurate and minimizing to individuals who are suffering deeply as a result of the very real truth that some people are very, very unwell.There are two kinds of relevant “crazy.” One is psychiatric illness—which I believe exists because I have seen it up close and personal, and I don’t believe demonic possession is the only cause. The second is often also psychopathology, but more firmly rooted in problems of personality functioning—identity, self-direction, empathy, and intimacy. It is the kind of crazy people make true crime podcasts about. The kind of crazy people make comedy specials about. The kinds of crazy that lead anyone to run for political office. Personality plus more traditional illnesses of the mind—psychosis, obsession, despair—these together create very serious problems for all of us. We can look at crazy—in the “what do you mean 30 emails an hour” sense, from a stalker—and simply call it “crazy” without understanding why, what, and how to respond most adaptively.We have problems that impact our wellness. We have unwell people who cause us all problems. Every once in a while it’s us—we have a psychiatric illness and find ourselves acting strangely, and worry—deeply—that we might be…you know, crazy.This newsletter strives to address both of these issues—we define mental health problems, and we will examine how brains and minds can conspire with the outside world to drive behavior over the edge for vulnerable people.It’s a newsletter about solutions to problems, second, and dismantling a crisis mentality first.

The Trial of Dr. Alan Emamdee I
The Frontier Psychiatrists is a newsletter and a podcast. Most people assume podcast means “recording a good enough conversation.” Yes, I do those too. I also have a sick fetish for spending way too much time crafting highly produced audio pieces that happen to be podcasts. I think these might need a different name in the future—what happens when species diverge in evolution?This story is about someone I know—Alan Emamdee, D.O. A man arrested for a crime he didn’t commit. Unlike the A-Team, he didn’t get to go on the run and help people unionize in an 80s TV show. He’s a doctor who suffered through years of a brutal legal process till he was acquitted at trial. The road back hasn’t been easy, but he had the tape. This is the first episode. It’s worth the listen. Please, share with your friends. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The End of Bromance
The Frontier Psychiatrists started as a Creator First show on the ill-fated clubhouse app. One of our favorite guests was the remarkable @Psych Fox (Jeremy Fox, LPC), an EMDR therapist with a passion for working with men around their actual problems. One of those is the loss of normative friendships among men—15% of men report no close friendships at all. This corrosion of close relationships is an accelerating problem for both individual men and society.Today’s episode of the podcast includes both the video above and pushes the audio to the podcast feed!Prior writing on the value of friendships and what we can do about that includes articles such as:It’s important to have FriendsFriends: A How-To GuideMatthew Perry was ClassyA Conflict of Interest Disclosure Regarding My Picks for SXSWThe Future of Brain Health?Announcing: May 5th, 2024…Rapid Acting Mental Health Treatment NYC 2024(Eventbrite Link)It’s a night of thrilling conversations about the future of mental health. It features speakers from…Videra, MDHub, Osmind, Neurosigma, iRxReminder, and…Lykos Theraputics!More info to come…but it’s the second IRL The Frontier Psychiatrists event, and we could not be more excited to have you! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

I Explained The Pandemic to Myself: Episode 5
The Frontier Psychiatrists is a daily health-themed publication. Your author’s love of podcasting is well established, and today, another from the vaults, dating back to the pandemic. In this episode, which I called “The Wave,” I started getting a little more ambitious in production, and strange in the jagged nature of my storytelling. I interview John Samuels, of WellWorth Advisors, Sonia Patel, of Capsule, and a journalist from the New York Times, as well as folks on my team at the time. Thanks for stepping in the way back machine with me. The pandemic was strange. It shaped us, now, and in the future. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
Change (Healthcare) My Mind!
I know how much my readers love my ongoing coverage of Change Healthcare, and sort of kind of promise to keep dissecting drugs or making fun of myself or whatever it is you find compelling about this newsletter and media empire. Today, however, I will publish a podcast. I had a conversation with @Psych Fox this week, before the ransom was paid, by UHC, about the Change situation. Out of respect to my guest, I’m going to publish it today. I also take requests on topics for articles and podcasts, so keep them coming. Thank you for reading and listening. If you are new to the newsletter, prior coverage of the change healthcare cyber attack is available here. and here. and here. and here. and here. and here. and also here. Oh, and with an NFT, here.An overview of all the things changed as is available in this article from yesterday. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Magnesium-Ibogaine in Veterans With TBI and PTSD
In this Frontier Psychiatrists Podcast, Jeremy Fox, P.C., And I discuss this remarkable work, as published by Cherian Et. Al. In Nature Medicine. Always love when @Psych Fox can pop in!We discussed the role of understanding the sample in a research trial and the remarkable potency of Ibogaine, with the additional safety of magnesium to prevent cardiac side effects, in this newly published research.Thanks for watching and listening, and feel free to share with your friends.Other excellent psychedelic-themed writers I’d highlight are Mason Marks at Psychedelic Week and The Microdose . Prior psychedelic medicine articles here on TFPs include:Are Psychedelics at Risk of Advertising Enforcement from the FDA?A Critique of “All Therapists of MDMA Assisted Therapy Should Take MDMA”Psychedelic Medicine for Primary Care?Dear Psychedelic Exceptionalism…William Osler, M.D., for Psychedelic Medicine Key Opinion LeaderPsychedelic Medicine Obtains Category III CPT CodesPsychedelic Medicine Needs to Get More Profit-FocusedI’m Psychic About Open Comment PeriodsWhy Medical Use and Spiritual Use Are DifferentPlease spread the good word—healing is coming, and more evidence is needed to understand when and for whom. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Can Employee Assistance Programs (EAP) be an On-Ramp for Help?
The Frontier Psychiatrists started as a “room” on Clubhouse, and in this podcast, I am joined by one of our favorite contributors @Psych Fox ! He joins me today to discuss how employee assistance programs can create the on-ramp to help and what might improve that process.A sampling of prior articles about employer-based health care is available here:The Science Behind The Best In Class Outcomes in Mental Health (with Acacia Clinics)Lawsuits for Health Plans Have BegunAlcohol Use Disorder is a DisabilityA Conversation About First Responder Health With Chuck DeSmithWhat is Health Insurance that is ERISA Compliant?Have Health Benefits Become a Huge Personal Liability for Employers?How Narrow Networks Can Win for Mental Health ParityCan’t Find a Psychiatrist? Now You Can Sue Your Company!Why Savings Claims Can Be A ScamWhat do Shaggy and Health Insurance Have In Common?Owen’s Letters to the Healthcare HackersI want to mention that another validated vendor in the mental health arena is joining my team at Acacia Clinics to have independent validation of our claims of being the best! I’m thrilled that my friends at Spring Health have achieved the coveted “savings validation” from Validation Institute!If you have been following the news of ERISA enforcement, this is important news. Employers need to get serious about providing better healthcare at a lower cost. Independent validation takes some pressure off when selecting the right vendors to make up a high-performing health plan. Why do I care, as a doctor, about health plans? Because great health plans are better for patients! Here on substack, Wendell Potter and Marshall Allen are on this beat as well, and I’d recommend a read! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Death of My Sister
On weekends, I tend to take a break from health policy to focus on personal writing here on The Frontier Psychiatrists. This one is unfortunate, and it is a fair warning to readers who are in no mood for something like that.My older sister, Alison, was troubled. She was also very gifted. She was trained as the chef at LaVernne, which was a very serious place to do your training as a chef. Parisian chef school doesn't f- around, and she was a gifted teacher of her craft. She landed a job that she thought would be great. Less work than teaching at a busy New York teaching school for chefs, the Culinary Institute of America. Something Downtempo.The Wexlers are incredibly wealthy people. She was a personal chef for Les Wexner. It was not an easy job. She is a personal chef for a fabulously wealthy person who is now notoriously on the list of individuals who are routine customers of Jeffrey Epstein. She wasn't just cooking for one person’s family. She was cooking for their hundreds of guests. She was one person. Her body couldn't take it. She had degenerative disc disease, and doing a job where she had to stand, endlessly, to cook hundreds of meals for hundreds of guests, as if one person could do all that by themselves, destroyed her body—destroyed her back. She ended up needing surgery. The surgery did not relieve her pain.After that back surgery, she was introduced to opiate pain medication. She has been prescribed a lot of opiate pain medication. And she took that opiate pain medication for years. She became addicted. She couldn't stop. The help wasn't there for the pain, and the fire she sent to her apartment that left her foot singed made the pain worse.Now she had chronic neuropathic pain from a fire that she sat in her apartment --the investigators told us that she had left a shoe on the stovetop. She was not well. She eventually reconnected with a friend, he became a boyfriend, he became a husband.For a while, he took good care of her. He had a problem also. In his case, it was with drinking. Her health was not excellent. This is often the case with burn victims. It's often the case with trauma victims. It's often the case with people addicted. It was the case with my sister. She was admitted to the intensive care unit, unbeknownst to me, three weeks after my father died of bladder cancer. She returned home. The next moment, as related to me, was probably after her last. She had survived a few suicide attempts already. There are only so many lives each of us has to spare.A phone call was placed to my mother by my sister's husband, letting her know that he found Alison in the bathroom, on the floor, not breathing. It was a fair question as to why the phone call was to his wife's mother and not to 911, given the not breathing... a subsequent call was placed to 911, and about an hour and a half of CPR took place, and like most CPR, the person did not come back to life. My sister was dead.The burial of my father and the burial of my sister were, unexpectedly, on the same day, in the same hole in the ground. I had lunch with my mother, my sister's husband, and others. We spoke well of her. We were sad. We all went about our days that followed.In her blood at the time of her death were the following compounds: olanzapine, Oxazepam, temazepam--both benzodiazepines--and heroin.She was also adopted. Her biological mother gave her away for adoption at age 14. She just didn't want her daughter anymore. If I had to guess the root of her pain? The event, the lesion, was this moment. Growing up, it didn't register how messed up this was. My mother adopted her. Her father was her father the whole time, but who switches moms? My sister, that is who.She posted this photograph of her and her mother on her Facebook, commenting that it was the last time she saw her mother, “20 years ago, and she was in a blonde phase.”It's not normal for your daughter to be given up for adoption. I have another older half-sister. That one? She wasn't given up for adoption. Just Alison. Not her older sister. This woman—whose name I don’t even know— gave away one child, not the other. It never mattered how much my mom loved her—my mother, who was her mother, which was a lot, frankly. How could you trust anyone wasn't going to leave you if your biological mother just dropped you from her life? It's hard for any child to understand the problem is factually with the parent. Healthy people don't do that. They are not so disconnected from their children that they pick and choose between them. That's not normal. That's not healthy. This is the kind of human Alison had as a biological mother. Our love for her? Perhaps it would never have been enough. The only thing that could fill that gaping hole was morphine, more morphine, heroin, oxycodone, Vicodin, more heroin, more Vicodin, endlessly until the end.I remember the last time we spoke—she apologized for being a bad sister. I reminded her that infinite forgiveness is what we are owed as family mem
Trauma Therapy You Don't Need To Talk About
I checked in with Jeremy Fox, P.C., about a new FDA-cleared device, the PRISM system by GrayMatters Health. This is a treatment modality for Post Traumatic Stress Disorder that doesn't require talking about your trauma! @Psych Fox is one of my favorite trauma therapists, so I called him to discuss.This is now offered at four sites in the US, and Fermata in Brooklyn, NY, is one of them. I discuss the experience of having PTSD myself and the role of trauma exposure in medical training and practice.I do the quick version of explaining the Prism System in 50 seconds here…More Jeremy Fox Themed Content:Bipolar Disorder: Myths BustedLSD for Anxiety?!: A PodcastPTSD and EMDR: A PodcastPeople I Mostly AdmireSome Other Content About Trauma:The ICU is Traumatic For EveryoneThe Once-Suicidal PsychiatristSo, Someone Has Been Stalking You?What Should Parents Say About Mass Shootings?Being Shot With a Gun is the Leading Cause of Death Among Children In AmericaA special thanks to the team at Graymatters Health, who visited our offices for deployment this past week! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Reading An Open Letter To My Bipolar Disorder
This article was among my most popular. Here it is, in podcast format. Enjoy!Other articles relevant to bipolar disorder include:DepakoteIs Bipolar Disorder a Circadian Rhythm Disorder?Lamotrigine (Lamictal) dosing guide.Does Lithium Prevent Suicide in Bipolar Disorder?Lurasidone (Latuda)Ziprasidone (Geodon)Risperidone (Risperdal)Why Don’t You Drink?Zyprexa (Olanzapine)The Time I Almost Set Myself on FireBipolar Disorder: Myths BustedThanks for listening, and consider becoming a subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

First Breaks
The Frontier Psychiatrists didn’t start as a newsletter. It began as a clubhouse room, with friends like @Psych Fox and Michelle Bernabe, RN joining myself and Carlene MacMillan, MD for audio-only conversations. Even before that, I was a bit podcast-obsessed. I won a grant to record podcasts about self-disclosure among health professionals at NYU—the Rudin Fellowship in Ethics and Humanities. This episode is built on a recording from that era—2017—with Gillian Waldorf, Ph.D. This is what I looked like way back in college:She is a classmate of mine from Amherst College, and we were both huge nerds who didn’t drink. Little did we know, we also had our first stirrings of psychiatric illness in common. This podcast is not perfect. It is also only part one. But perfect, as this newsletter + associated media is fond of embodying, is the enemy of the done. This was recorded, edited, and scored by yours truly, Owen Muir, M.D.I hope you enjoy it. Please share and review on Apple Podcasts if you do! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Remind-er! An Interview with Anthony Sterns of iRxReminder
The Frontier Psychiatrists is a substack-hosted media empire…we have video, newsletter, dumb memes, podcasts, and music—my gosh golly! Today, I bring you a conversation with a colleague who is both humble and brilliant. We first met on Clubhouse—in 2020—when Carlene MacMillan, MD and I were hosting conversations on the weekly. Tony and I met again in the What If Ventures fellowship, and, as I have told him, we just enjoyed each other’s company. We collaborated on grant writing, and one thing led to another…and now I’m the Chief Medical Officer of his company, iRxReminder. Anthony is a kind and funny person to work with, which I couldn't value more highly. He is also brilliant. He understands medication adherence problems better than anyone I’ve ever encountered. In this long overdue podcast, he explains the problem and how we address it with our closed-loop AI + Internet of Things cognitive prosthesis. He’s a master educator, friend, and my CEO (in one of my gigs)! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

"Can Anxiety Can Be Over?": MM-120, an LSD Analog Phase IIb Data in Generalized Anxiety Disorder Released!
The Frontier Psychiatrists started as a room in Clubhouse, and one of the people who made that awesome was Jeremy Fox, P.C. He joins me today for this video podcast to chat about the groundbreaking phase IIb data released by Mind Med today:MM-120 100 µg – the dose achieving the highest level of clinical activity – demonstrated a 7.6-point reduction compared to placebo at Week 4 (-21.3 MM-120 vs. -13.7 placebo; p“We are excited by the strong positive results for MM-120 in GAD, particularly given that this is the first study to assess the standalone drug effects of MM-120 in the absence of any psychotherapeutic intervention. These promising findings represent a major step forward in our goal to bring a paradigm-shifting treatment to the millions of patients who are profoundly impacted by GAD,” said Robert Barrow, Chief Executive Officer and Director of MindMed.”Jeremy and I discuss MM-120, SAINT neuromodulation, and why BIG effect size interventions that work fast matter in Medicaid populations!Thanks for listening!The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Ramon Lizardo, M.D. talks Disability, and Raising Your Kids Right
Ramon Lizardo, M.D., and I met at least two years ago when he was an investor, and I was pitching him… something. We’ve become friends. In this conversation, he reveals that while he was busy building fabulously successful healthcare companies, he was also going deaf. The audio isn’t great…which I am going to consider “irony” kicking my ass. But he’s a fascinating human, and I’m a big fan. It ends with some remarkable insights into parenting. Thanks for joining the Frontier Psychiatrists today! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Future of Brain Health?
Welcome to the Frontier Psychiatrist…. Podcast. It's a podcast with myself, Dr. Owen Muir, as your host, and it's a companion podcast to FrontierPsychiatrist.com, a sassy Substack about health-related things. This is a conversation between Jazz (Glastra) and me. She is the senior director at Brain Futures, which is a 501c3 not-for-profit. She got to be the interviewer in this one! I’m a big Jazz fan, as a person, in full disclosure. I also enjoy the art form of the same name, but that is a different story.We are thrilled to have BrainFutures as partners in sponsoring Rapid Acting Mental Health Treatment 2024. It’s in San Fran on the 7th of January! Join us! (that is a ticket link!)In this conversation, we try to get to a shared understanding of what we actually might mean by mental health, the mental health crisis, and whatnot. This means accepting that other people's minds might not be thinking the same things that we're thinking, and so trying to get to the same understandings is a process that we have to take seriously. We need to build trust, and that's really, at the end of the day, what this conversation is about. The transcript follows…Jazz Glastra I'm Jazz Glastra, and I'm the Senior Director at Brain Futures, which is a nonprofit that advances access to new treatments and technologies in brain health. Owen Muir, M.D.I'm Owen Scott Muir. I'm a child, adolescent, and adult psychiatrist by board certification. I identify as an interventional brain medicine doctor because I don't really love... the branding of psychiatry or the expectations. Much of this goes back to me constantly thinking about the role of trust and expectations in any conversation. Jazz Glastra What is the difference between a neurological disorder, a psychiatric disorder, and a neuropsychiatric disorder?Owen Muir, M.D.In the beginning, there were only humors. And that's a little bit of a joke, but We had neurology as a medical specialty,Sigmund Freud, whom we think of as a psychiatrist, was a neurologist. Because we didn't have psychiatry as a separate medical discipline, to this day, the American Board of Psychiatry and Neurology is one board, ABPN. What ends up in what bucket in medicine has a lot of historical ness to it? Neurology used to be all of it? If it was a brain or a nerve, That was neurology, and then Freud came along with an explanatory model for problems people had that didn't involve localizing the lesion,? Neurology took over things where you could point at where it was, and psychiatry took over things where you couldn't point at where it was. If you end up having a thyroid problem, then you go to endocrinology, and you're not managed primarily by psychiatry. The accident of history is nonlocalizable Neurology ended up as psychiatry.And here I am, talking all the time about fMRI-guided treatment, so I'm getting myself in trouble. One of the people who brought this bridge back was Dr. Nolan Williams, who trained initially as a neurologist. He did neurology first, then got board certified in behavioral neurology, and that not being enough residencies, he did an entire other residency in psychiatry.And three board certifications in, he's a neurologist and a psychiatrist, and blah blah blah. It ends up being, “Who's got the most practice in their training program with whatever the problem is to own it.” It's an accident of history is the answer.Jazz Glastra So, are we in a mental health crisis?Owen Muir, M.D.Yes, in that we have no idea what that means, and we feel very crisis-y about it.Jazz Glastra I feel crisis-y about it, usually.Owen Muir, M.D.What is mental health? I have no idea. It is the worst term because it means nothing. Which is really good for charlatans and hucksters and bad for people who are suffering. I would agree we're in a mental health crisis if, in the same question, you let me say, are we in a mobility crisis?Yes. When we only fill cars with water that should have taken gas, that's a mobility crisis, and we can have the same response to the mobility crisis of filling up gasoline-powered cars with water as we do to the mental health crisis. I'd say those are similarly crisis y. The cars wouldn't move.And you could talk about what a problem it was all day long, but the car still wouldn't go because you filled it with water, not gas. That's how I think of the mental health crisis. It's a crisis of misunderstanding; the problem is you don't understand the problem, and then you don't apply the right solutions, and you act like it's a crisis, not an actual understandable and solvable problem.Jazz Glastra What do you see as the problem?Owen Muir, M.D.If you don't know what a mental illness is, or that there are different ones, and that's important, is there a problem with people who are, for example, dying by completing suicide? Yes. That is one version of looking at the problem.Is there a problem with people having tremendous suffering? Needlessly throughout their day. Yes. Is there a problem of people

PTSD, EMDR, and TFPs: Jeremy Fox, P.C. Joins for a Conversation About Trauma Therapy and The Brain
The Frontier Psychiatrists is a health-themed media empire(!) with a newsletter as its home base here on Substack. It started as conversations on the app Clubhouse, and one of our—Owen and Carlene’s— earliest friends is Jeremy Fox—a licensed professional counselor. He’s a specialist in trauma, an EMDR trainer, and a great explainer of things complex. I also think he is a decent human I love talking to. In this interview, we dig into the neuroscience of EMDR—eye movement desensitization and reprogramming—for trauma and more. Please share with your friends, and give the show a follow-up and 5-star review on Spotify, Apple podcasts, etc.Here is us with the lord of Winterfell, given Winter is Coming. He needs a better coat. Advertising For Other Things Section!I work at a practice in NYC for those interested in neuromodulation-first approaches to mental health problems. That means not drugs. It’s called Fermata. We are enrolling for the fMRI Guided Depression Trial: The SAINT OLO Study! If you are interested in the treatments we discuss, you can either become a patient or enroll in a research trial, depending on what is right for you. A note: Some of our trials (like SAINT) require payment from patients, and we pay you for others (like TDetect). This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Fire Chief and the Psychiatrist: A Conversation with Chuck DeSmith
Chuck DeSmith is a remarkable man—a King County Firefighter, innovator, and a delightful person for a great conversation. Video Version also available on YouTube channel! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe