
The Frontier Psychiatrists
102 episodes — Page 2 of 3

I Explained The Pandemic To Myself: Episode 4
I’m Owen. This week of posts is different from the usual…it’s a bit of an origin story for this newsletter, The Frontier Psychiatrists. It’s a daily health-themed newsletter by Imperfectionist physician Owen Scott Muir, M.D. There is a podcast (this), videos, a therapy training book, chapters in other therapy manuals, some poetry books, a live event in January, and even a brain-stimulation first clinic in NYC where your depression can be treated in an open-label clinical trial—to remission in 79% of people—without drugs or talk therapy.How did all this come to be? That is what this week’s series of podcasts are the slow-roll story of!It all started with a podcast about the pandemic. For those listening closely, the last episode was from March 22, 2020. This podcast was recorded the NEXT DAY, on March 23rd. Michelle Bernabe, RN believed in me, and we all need that. Michelle and I were working together at a practice at the time, and the pandemic hit. She is the person who taught me about the hero’s journey and narrative structure. She encouraged me to keep telling a story. The story was about the pandemic at the time. This episode is based on an interview with a nurse struggling to endure the horrors of the early pandemic in New York. As it relates to this newsletter and your author, the story is about the dates. Episode 3 ended, and I was recording Episode 4 the next night. I was dropping perfectionism in the heat of the moment and striving to tell stories that didn’t have to be perfect..I am, by necessity, becoming an imperfectionist. There is no perfect in a pandemic. It’s chaos, and perfection stopped being an option.This week’s articles tell the story of how I got to write a daily imperfectionist manifesto by showing you how I started telling imperfect stories.Your feedback, dear readers, is welcome! Thanks for listening, and stay tuned for the next thrilling episode, where I get a bit more ambitious and fall off the wagon a little. It’s not a linear journey!Plug 1: I work at a practice in NYC for those interested in neuromodulation-first approaches to mental health problems. That means not drugs. It’s called Fermata. We are even enrolling for the SAINT OLO Study! Plug 2: Tickets are available for the Frontier Psychiatrists live event: Rapid Acting Mental Health Treatment 2024, Jan 7th, in San Fransisco! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

I Explained the Pandemic To Myself: Episode 3
The Frontier Psychiatrists is a health-themed newsletter and podcast. It’s a little bit of a media empire; there is a YouTube channel, Instagram, TikTok, and music I do over on Spotify up top. This article is a bit of a meta-article on my journey, with historical audio as reference material.I’m Owen Scott Muir, M.D., and I’m prolific, if nothing else. My first pass, as it were, at content creation was more plodding because podcasts—after music—were my first love. I consider myself an imprefectionist, now. This is a maxim for me—the done imperfectly and on to the next iteration is better than the perfect. One of the perils of podcasting is my fancy taste—I love Radiolab. I have Radiolab production alumni in my life. I love craftsmanship in a production! The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.The flip side is I am one person. Who isn’t perfect? Believe it. This person—the modern imperfectionist version of me—has had guides on getting more iterative things done. One is featured in the podcast attached to this very set of words. It’s my friend Michelle Bernabe, RN who writes Moral Health ! My mom is also in this episode.Enough preamble, now to the prologue. My journey to imperfection as a maxim began with the hero’s journey. I was in the ordinary world—pre-pandemic, and then there was the call to adventure. Except there was nowhere to go and nothing to do. Cause there was a pandemic. I started getting less-than-perfect content out in the world. This is the third episode of that “body of work.”Michelle—a nurse with whom I worked at the time— and with whom I am still proud to call a friend today, taught me about narrative structure and the hero’s journey. She had a very dear friend teach her the same lesson. Slowly, I began to realize the hero’s journey I was on was as a storyteller myself…and the story I was telling was both about imperfectionism and in an imperfect format.Much of that story will later be told, over and over, on the Clubhouse App in late 2020…but at this point—the March 19th date on which I recorded this podcast was subsequently released on March 22nd. That is a quick turnaround.I am trying to understand the weirdness of the pandemic, yes. I am trying to understand how to communicate about public health. I am scared; you can hear it. But I also got a thing done and then another. I am starting to let go…to get going.This is episode 3. It’s an origin story of a sort!Plug 1: I work at a practice in NYC for those interested in neuromodulation-first approaches to mental health problems. That means not drugs. It’s called Fermata. We are even enrolling for the SAINT OLO Study! Plug 2: Tickets are available for the Frontier Psychiatrists live event: Rapid Acting Mental Health Treatment 2024, Jan 7th, in San Fransisco! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

I Explained the Pandemic To Myself: Episode 2
The frontier psychiatrists is a Substack written by Owen Scott Muir, M.D.—a child and adult psychiatrist. This podcast is shared from the vaults…here is the story.I live in Brooklyn, New York. For those who remember 2020, we had a pandemic! I know, right? Ancient history! This is audio archeology. I did what I like to do to calm down to cope, which is I started recording stuff. That stuff became a short-ish run podcast, which I called “Remotely Possible: Uncertainty, Anxiety, and Existential Despair.” Was it content marketing for the end of the world? Regardless, it is, in retrospect, a strange time capsule about how I was thinking about the pandemic at the time, and I think it holds up pretty well. The uncertainty of that time was defining.In retrospect, listening to these podcasts, given everything we know and all the things we don't…My bottom line? Uncertainty is hard for us as humans. We're deeply unsettled by the uncertainty. We’d rather things be sh*tty than unclear. We strive to make things bad when we have uncertainty because it's easier than sitting with it. And, frankly, this makes some sense to me. We are not completely irrational — it's avoidance behavior. People avoid things that hurt. People avoid things that suck. One of the things that hurts and sucks is uncertainty. Thus, there's some degree of predictable behavior from humans when things are uncertain. They're going to take the path of most certainty. Even if that path sucks. My issue with the pandemic response ended up being around creating a primrose path straight to hell, which may have been a trap we didn't need to leave for ourselves.We wanted the certainty of what to do—even if it was sometimes dumb. We wanted a vaccine that would be perfectly efficacious—which doesn’t exist. And perfectly safe. Which doesn’t exist.We are predictable. We will avoid “not knowing”— if we don’t build trust first. The pandemic was a giant trust fall that went south cause we forgot about the trust building, in retrospect. With that musing…I hope you enjoy episode two of my pandemic retrospective.Plug 1: I work at a practice in NYC for those interested in neuromodulation-first approaches to mental health problems. That means not drugs. It’s called Fermata. We are even enrolling for the SAINT OLO Study! Plug 2: Tickets are available for the Frontier Psychiatrists live event: Rapid Acting Mental Health Treatment 2024, Jan 7th, in San Fransisco! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
I Explained The Pandemic to Myself: Episode 1
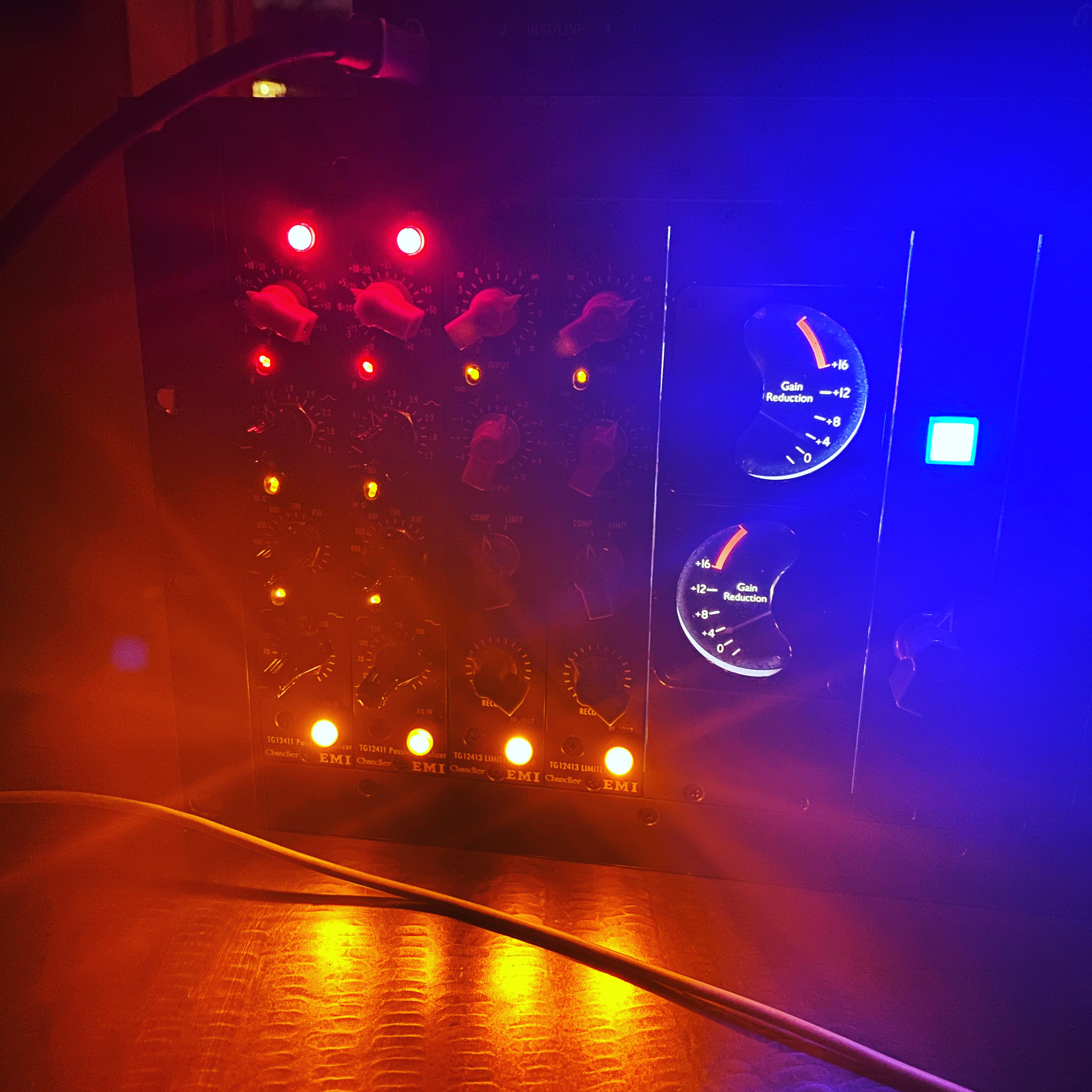
In the pandemic, I didn’t know what to do with myself. One of the things I did to make sense of my world falling apart was to make a podcast. I think the questions I asked at the time hold up well enough. This is the first episode I made, just about a week into lockdown in New York City. I recorded the audio on March 13th and released it on March 15th, 2020.Frankly, the worst thing about how we handled the pandemic was how we explained things—and this lack of focus on mistrust engendered as a public health risk is an enduring legacy. I called the show “remotely possible.” This is a photo of the first recording setup on my kitchen table.Let me know what you think, with the distance we have now. There are more of these. I’ll release them in this feed.Thanks for reading and listening. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Complex Case Psychiatrist
This is an interview from 2015 with Samuel Sharmat, M.D., a brilliant diagnostician. It also was an interview that, in retrospect, helped define my options as a physician. He has a traumatic brain injury as a young child, it changed him. For him, the change unlocked new ways to notice what might be wrong with patients in ways that others could not. Please listen, and share with your friends. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Once-Suicidal Psychiatrist...A Self-Disclosure, Deferred.
I won a grant years back to produce a podcast series from NYU’s Rudin Master Scholars Program in Ethics and Humanities. I am proud of that work. This episode never made it on the air. It is presented for your consideration. Suicide is discussed, frankly. Both my friend and guest, Lara J. Cox, M.S., M.D, and I discussed extensively that her name should be used. That personal disclosure was the healing element, as we understood it.I presented this work on May 6th, my birthday, in 2018, at the APA annual meeting. That morning, a psychiatric resident in a local program died by suicide. It was devastating. This is a challenging disclosure to write— because of my worries about contagion effects. This issue around contagion was the difficulty in editing these stories to begin with.These stories aimed to REDUCE suicide risk by providing stories of hope. These stories offer support for vulnerable medical trainees. Otherwise, they learn the lesson…as part of the hidden curriculum of medical training: “It’s unsafe to talk about your struggles, even in the past.”We lose hundreds of physicians to completed suicide every year, and the numbers on ideation are dispiriting:A 2015 meta-analysis of 54 studies examined the prevalence of depression and depressive symptoms in resident physicians across decades and around the globe.2 They found a 15.8% increase in depressive symptoms during the first year of residency, across all specialties and countries of training. Over the course of training 20.9% to 43.2% of residents reported depressive symptoms, with symptoms increasing over time. This finding could be extrapolated to fellows, attendings, and other post-training physicians. Currently, the actual data for post-training programs is sparse. When we refuse to speak—using best practices—we are also heard. I have long argued this is not the way.The physician interviewed in my podcast above is brave, outspoken, and a personal hero. Lara J. Cox, M.S., M.D., has served on the Board of Trustees of the American Psychiatric Association and is herself a scholar of suicide prevention. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Psychiatric Nurse...who was once a State Hospital Patient
I won a grant years back to produce a podcast series from NYU’s Rudin Master Scholars Program in Ethics and Humanities. I am proud of that work. Here is one of the episodes that NYU “Doctor Radio” felt was a touch too edgy…I’d love to make more, but this production isn’t cheap!Thanks for listening, and share with your friends—a special thank you to Lancy Levy, R.N., my guest in this episode. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

What Happens When You Make Perfection... a Failure?
The Frontier Psychiatrists is a newsletter. It's written by one Psychiatrist, Owen Muir, M.D. It's a health-themed newsletter. It's also an exercise in imperfection. That imperfection is not an accident. Here is the story…An influential book in my life? It is not about medicine. The book is called Measure What Matters. It is by John Doerr; you can buy it on Amazon with that link! John writes about the system called objectives and key results (OKRs). Andy Grove originally developed this management and goalsetting methodology at Intel.I think it's a meaningful bulwark against perfectionism. It is a philosophy. OKRs are a system for setting measurable goals. But—there is a quirk. This quirk makes it different—and more powerful— than other goal-setting approaches. The system works as follows: * set an overarching objective, and the point is to be audacious. I'll give you a very real-world example:“I'm going to write a great health-related newsletter (all by myself) that influences people’s decision-making towards a better future.”Now, here's the trick: you have to figure out how to determine if you're moving toward that goal. And it has to be measurable. When you start this process, you don't necessarily know the best way to measure things for yourself or a larger organization; this is the scaffold.There are rules: * At the end of your audacious goal, you add the statement: “as measured by:”Next, you limit yourself to between two and three (easily) measurable key results demonstrating that you are appropriately pursuing that goal. The quirk is* if you achieve more than 70% of your key results in any given quarter, you did it WRONG. Getting it perfect means you didn't get it RIGHT.My God, right?This is a system to learn how to set audacious goals! I could've set my goals for this newsletter— and did— as follows: “as measured by… publishing an article every single day.”That is a “key result.”This is not the same as a key performance indicator (KPI). Key performance indicators are measurable. Some, however, are all or never—you don’t want to close 70% of surgical wounds! Many things are measurable; not all KPIs are useful tools in this OKR framework.All Key Results are KPIs; not all KPIs are suitable Key Results for your strivings.I write an article almost every single day. I will calculate that for my readers at the end of this quarter, and you can see how I did. I didn't know what key results were the best way to build an influenced audience with this newsletter. Did I get it wrong with this key result? First, I have achieved the goal more than 70% of the time! I underestimated the difficulty, and thus the audaciousness, of a daily one-person newsletter for me as a writer. By writing a daily Health-themed newsletter, I failed to be audacious enough! Or I didn’t select the right tools with which to measure. I would probably want to set another key result to guide me when I revisit the original goal and its measurement. Which is very much the point. OKRs are not “set and forget”. They are set and revisited. It’s an iterative process. We learn, with OKRs, that successfully striving is the meta-goal. We know if we succeed by measuring iteratively, and in failing to be perfect, we learn the right degree of stretch in any epoch.Perfection is imperfect. Striving is a learned behavior and a set of skills. Not always striving is an easy way to avoid the audacious. In my example, my daily publication schedule might not be the best way to achieve my goals.I’d have to find a better way to measure. Repeat.Perfection is poison for those who wish to strive. To succeed at striving is to fail… the right amount, over and over. OKRs are an antidote to the hopelessness of perfectionism and the fragility of narcissism. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

World Mental Health Day
Do you have any idea what mental health is? I wish I did. You have permission from me to be confused. I’m Owen Scott Muir, and I’m a Mental Health Professional. I should probably have an idea. I refer to the Frontier Psychiatrists Substack as a Health-themed newsletter for all the reasons I’m going to enumerate. Subscribe. We've been told mental health is important. It is. I don't know what the word it means in this context. Or I would like to know if we have a shared understanding of the word we would accept be acceptable in any other conversation. If we ask if your car is OK, we have a general sense that the car would need to have:* structural integrity, * four tires, * the ability to move on those rolling tires from one place to another, * not breaking down constantly, and * not crashing into a wall. Working tires, wheels, and the ability to move someone from one place to another are all accepted concepts regarding the utility of anyone's car. Cars need to go… safely.Health, as a more broad term, is better understood. Are you actively dying? Are you in pain? Are you able to breathe? Is your heart beating? Can you get out of bed, comb your hair, brush your teeth, go to work, and hug your children? Activities of daily living have been defined.I fear we made a mistake by putting the word mental in front of the health. It's confused us. Because it suggests there's something different about mental health and health. Health, the state of well-being in which one can do the things they need to do in the day without significant impairment, is a meaningful way to assess whether someone's health is good enough. Being functional, you don't need the word mental in front of it.I would encourage us to consider Health on this World Mental Health Day. I would encourage us to think about the distinction between disability by any standard and what would be the ability to do life things by any measure. The brain is part of the body. The health of the brain and its relationship with the body matters. Similarly, the health of your body and the health of the bodies and brains of the people you interact with matter.I urge researchers and clinicians to look at ability and disability broadly. * Are you able to focus? * Are the things on which you can focus the things you'd like to focus on? * Can you have positive, loving relationships in your life? * Can you do meaningful work? * Can you pursue a goal? * Can you imagine feeling satisfied? * Can you work towards feeling satisfied, perhaps in an accessible educational setting?The further we get from the confusing specifier of mental before the word Health, the better. It is about addressing disability. We happen to have laws about that, at least in the US.Healthy people are mentally healthy people. Being mentally healthy doesn't do much to add relevant context, and I fear that it subtracts some from our ability to understand each other.Thanks for joining me on this World Health Day, which is maybe what we call it in the future. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Neuroscience of Fear
This is an episode of the Frontier Psychiatrists Podcast. It’s a conversation between my Fermata team member, Chelsey, and Myself. This conversation is about us, at work, trying to understand neuroscience together. We recorded this one! An edited version of the transcript follows.Owen Muir, M.D.: So we were chatting about the amygdala, and if you want to ask me any questions about it, I can answer them and edit it together. And that's a podcast. Chelsey Fasano, BA: There's a lot of discussion in the field right now about location neuroanatomy or chemistry neurobiology. And I'm always thinking about how the two crossover, so we're talking about the up-regulation or down-regulation of the amygdala.What are the neurochemical aspects of how the amygdala would be up- or down-regulated?Owen Muir, M.D.: Neurochemistry is a great way of selling drugs and selling explanations that are easy to understand.When we talk about neurochemistry, we're talking about a synapse between two nerves that are trying to communicate. There's a tiny little gap, and the way a nerve communicates with another nerve cell is a neurotransmitter is released from one and floats its way across a tiny little gap, and then hits a receptor on the other side, and that creates a change in that subsequent cell, which makes it either more likely or less likely to fire.What's happening next is within that cell. There are intracellular changes that lead to an increasing likelihood of reaching an action potential and itself firing and effectuating the next change in its neighbor cells. We focus narrowly on neurochemistry, because we can look at and modify it.We're getting obsessed with answerable questions— not with important questions. For example, we don't give people “hyper-glutamate,” the excitatory neurotransmitter in the brain. They'll have a seizure. Those excitatory impulses open ion channels that cause immediate depolarization and firing of neurons. Uncontrolled depolarization leads to seizure and death. GABAergic drugs do the opposite thing. So, anything binding to the GABA receptor opens a chloride channel. Chloride's negatively charged.And that changes the inside of the cell's voltage to negative, which means it's less likely to fire because you need more glycine and glutamate to increase the voltage. GABA is safe to agonize, because you're not going to get a seizure—but withdrawal is dangerous because now you're more likely to fire in the absence of the GABA drug.We're focusing on other compounds like serotonin, norepinephrine, and dopamine, which functionally regulate the internal cellular environment, making firing more or less likely. And we focused on it because it's safer. We got obsessed with what we knew we could do and not immediately kill somebody— as opposed to what might actually be effective or is happening naturally because, on their own, our cells are firing and releasing neurotransmitters and pulling them back up and regulating their voltage without us messing with it at all.For example, the chemistry argument at the amygdala level is part of the story. But when we're talking about what information the amygdala is kicking out, it's really how fast it is firing. That's my kind of argument. It's a rhythm answer. If we looked at the stage plot for AC/DC and saw they had a lot of cables and started worrying about which cable plugged into the guitar as opposed to they are going to play in time --and you can replace the strings, the guitar, the cables. You do not have a good AC/DC show if they play at a time, and if they're playing in time, even if the guitar cuts out like bass drums, Angus is still locked in, and it rocks.We've focused on what's focused-on-able, not what matters.Chelsey Fasano, BA: The primary neurotransmitters of the amygdala are precisely the ones you were talking about!Owen Muir, M.D.: The n methyl D aspartate receptor is a binding site that modulates glutamine.Chelsey Fasano, BA: So that makes sense as to why ketamine would strongly affect PTSD since it works primarily on NMDA and GABA. That would downregulate the amygdala, which would help to buffer against the overactivity associated with PTSD and subcortical areas.Owen Muir, M.D.: The firing rate functionally comes down because each nerve in the amygdala firing becomes less likely by some amount. Chelsey Fasano, BA: Is the feeling something to this whole hippie thing of vibration and vibe?Owen Muir, M.D.: It's true at the level of the neurons in the brain. Yes. I think wavelength is an accidental term. I don't know. But it's the literal truth.Chelsey Fasano, BA: We know that neural firing from some research that I've read affects motor movements and speech patterns, and so there probably is some truth to the fact that upregulation of specific circuits is going to cause speech pattern and motor movement differences that are going to be the bodily rhythmic reflection of the brain activity. We would pick up a vibe because we all sense those things about each

Schizophrenia Is More Dangerous Than A Car Crash, and Treating it Saves Lives
The Frontier Psychiatrist's newsletter? It is what you are reading. It’s a health-themed publication written by Owen Scott Muir, M.D. This is a brief detour from my recent series on medications, many of which have a critical slant. Those include Risperidone, Depakote, Geodon, Ambien, Prozac, Xanax, Klonopin, Lurasidone, Olanzapine, Zulranolone, Benzos, Caffeine, Semeglutide, Lamotrigine, Cocaine, Xylazine, Lithium, dextromethorphan/bupropion and Adderall, etc. I write this all by myself every day. Consider subscribing. (the paywall starts 5 weeks back, and there are 360something articles back there). It makes a horrible or awesome gift, depending on your friend circle. I also get paid more money by Amazon if my readers buy stuff now, like, for example, my favorite book about mental illness—or this tea I drink daily. I also encourage you to send me this coffee maker— or, more realistically, to anyone else.Today, I address what happens when schizophrenia is not treated, even if it is. It has high morbidity and mortality, a problem that medications address. Effectively. Not without costs, but the best data suggests treatment is better than no treatment for most people.I’m going to cut to the chase briefly, and if you or a family member want to read a great book on treatment with antipsychotic medicine, I’d recommend this one. Jeff Leiberman, M.D., has been …controversial… of late. However, there is no denying his role in understanding schizophrenia and its treatment, and his book on the topic is worth a read or listen, called a Malady of the Mind.Psychotic. We use the word commonly in chit-chat to denote something is bad. Unreasonable. Wrong. Deranged. Nothing is beguiling about the word. It is a thing to deny in oneself— “I am not psychotic!”Understanding PsychosisSome people don’t get that luxury. Some people are honest-to-goodness psychotic. Most of us do not know what that means. Some of us do, and some smaller portions are blessed with the ability to spend time on both sides of that psychotic equation. I will define the term:Psychosis refers to a collection of symptoms that affect the mind, where there has been some loss of contact with reality. During an episode of psychosis, a person’s thoughts and perceptions are disrupted and they may have difficulty recognizing what is real and what is not. The most common illness we associate with psychosis is schizophrenia. Psychosis can occur with depression, bipolar disorder, and other maladies. Depression and mania are mood states; we refer to these mixed with psychotic symptoms as affective disorders in psychiatry. A brief grammar note, brought to you by Grammarly, a tool I use and—sadly—am not paid to promote:Is affective just another word for effective? Are the two words similar and entangled in the way the verbs affect and effect are? No, affective is not just another word for effective. And affective and effective are not derived from the verbs affect and effect. They come from the nouns affect and effect.There is a difference in the literature—and in the lives of patients—when it comes to illnesses that have affective psychosis and non-affective psychosis. Much of the anti-psychiatry crowd focuses on affective disorders and argues about the side effects of those treatments. Less attention is paid to non-affective psychosis because It’s not as compelling an argument. These are challenging illnesses either way and are associated with significant morbidity—impairments in life—and mortality—early death.“Uncured of Worse”: 1937.As far back as 1937, authors noted the grim prospects in the long-term course of schizophrenia (in this context, I’m referring to largely “non-affective psychosis” —where the delusions or hallucinations are not tied to mood episodes):Of the 100 cases, 66% were uncured or worse after the lapse of 6-10 years, with persisting process symptoms or in a defective state after the course had run; 13% were improved, 4% were cured with defects, and 17% were completely cured. “The Prognosis is Poor”: 2010By 2010, with decades of more data, the conclusion was much the same—schizophrenia sucks, even compared to other admittedly bad illnesses:Our 26-year longitudinal study and other longitudinal studies confirm older views that outcome for schizophrenia, while showing some variation for different schizophrenia patients, is still significantly poorer than that for other psychiatric disorders.A large NIMH follow-up study with 2 to 10 years of time following patients from a first episode that required hospitalization demonstrated:The sample showed substantial functional impairment and levels of symptoms, with only about 20% of the sample demonstrating a good outcome…The “not-good” outcomes looked like this:78% of the sample suffered a relapse, 38% attempted suicide and 24% had episodes of major affective illness.Beyond Psychiatric Problems?We tend to focus on the role of bad psychiatric outcomes as psychiatrists. Still, the medical outcomes are similarly

Risperidone
My favorite opening line of an academic article (this week) follows:Mental illnesses are prevalent, cause great suffering, and are burdensome to society.Welcome to the Frontier Psychiatrists. It’s a newsletter that I write all by myself. I’m doing a series on medications, largely (but not entirely) in psychiatry. I’m a child and adult psychiatrist, and I still see patients. I’ve also been a patient since I was 16 years old. Please consider subscribing and sharing widely.The first antipsychotic introduced after clozapine would be a big deal—especially if it didn't cause life-threatening side effects. Risperidone was first developed by the Johnson & Johnson subsidiary Janssen-Cilag between 1988 and 1992 and was first approved by the FDA in 1994. It’s one of the very few drugs with data for bipolar disorder that I, personally, have never been prescribed.Risperidone—Risperdal as a trade name—was ready to be a huge hit.It was presented as very atypical—this was the post-clozapine branding of choice. The “second generation” label was added years later. I have a confession to make. After residency, when the attending doctors told me, as a trainee, what to prescribe, I never prescribed risperidone ever again. I think this compound—and paliperidone, the metabolite— still has an important role in managing schizophrenia and bipolar disorder. There are more formulations of long-acting injectable risperidone and related compounds than I can remember. I think those are going to be useful drugs for a long time. Oral risperidone? Nope.Clozapine was an exciting drug. No horrible motor side effects? (Plausibly) More effective? It was better than every drug that came before. It had this pesky adverse effect that could lead to death called agranulocytosis, which I addressed in my first research paper in 2011. We needed more drugs that were this atypical!We—the field of psychiatry, at least— needed things that were not gonna kill you abruptly, in a terrifying manner, like clozapine had the rare potential to do. But we didn't want more of the same old antipsychotics. After Psychiatry got a taste of not having to explain permanent tardive dyskinesia as a likely side effect of antipsychotic medication, we wanted to keep doing that. Editors note: It is still a side effect of all non-clozapine antipsychotics, and we should never have let our guard down.Risperidone was the first antipsychotic that came to market after clozapine rocked the world of psychiatry by being better. Risperidone is similar, and they even use the accidental branding of clozapine— “atypical”—for this medication. The Food and Drug Administration (FDA)-approved indications for oral risperidone (tablets, oral solution, and M-TABs) include the treatment of:* schizophrenia (in adults and children aged 13 and up), * bipolar I acute manic or mixed episodes as monotherapy (in adults and children aged 10 and up), * bipolar I acute manic or mixed episodes adjunctive with lithium or valproate (in adults)* autism-associated irritability (in children aged 5 and up). Also, the long-acting risperidone injection has been approved for the use of schizophrenia and maintenance of bipolar disorder (as monotherapy or adjunctive to valproate or lithium) in adults.The “mechanism of action” of all of the drugs that have efficacy in psychosis was presumed to be dopamine D2 receptor blockade, a mechanism shared with all of the prior medication from Thorazine (chlorpromazine) through Haldol (haloperidol). The assumption—which clozapine disproved—was motor side effects were required for the drug's efficacy in psychosis. This primacy of the D2 blockade as a mechanism of action has since been disproven. This is the mechanism that leads to gynecomastia, leading to a bevy of lawsuits from men who developed breasts. It also causes related side effects like galactorrhea—breast milk from breasts that can be on men or women who are not nursing— and erectile dysfunction. Dopamine—it does a lot of work in the brain, not just pleasure.This motor side effect profile was not true with clozapine. It had various additional receptors, particularly in the serotonergic family (5HT-2a, for example), and alpha-adrenergic, histaminic, and other receptor sites throughout the brain. This broad profile of different receptors explains the wide range of side effects. But more importantly, these are complex, “messy,” and hard-to-predict outcomes given the complexity of the brain. The complex pharmacology allowed psychiatrists like me to think—hard!—about which particular witches brew of receptors we would choose to tickle (agonize) or antagonize. It’s very satisfying. I also suspect this is a story we tell ourselves that is not as closely moored to truth as we’d like. We enjoy thinking about science-ish stuff. Receptor binding profiles are seductive— because they are knowable. Our patient’s heart, hope, dreams, and heartbreak? Less so.The most important feature of risperidone today—and its 1st order metabolite, pal

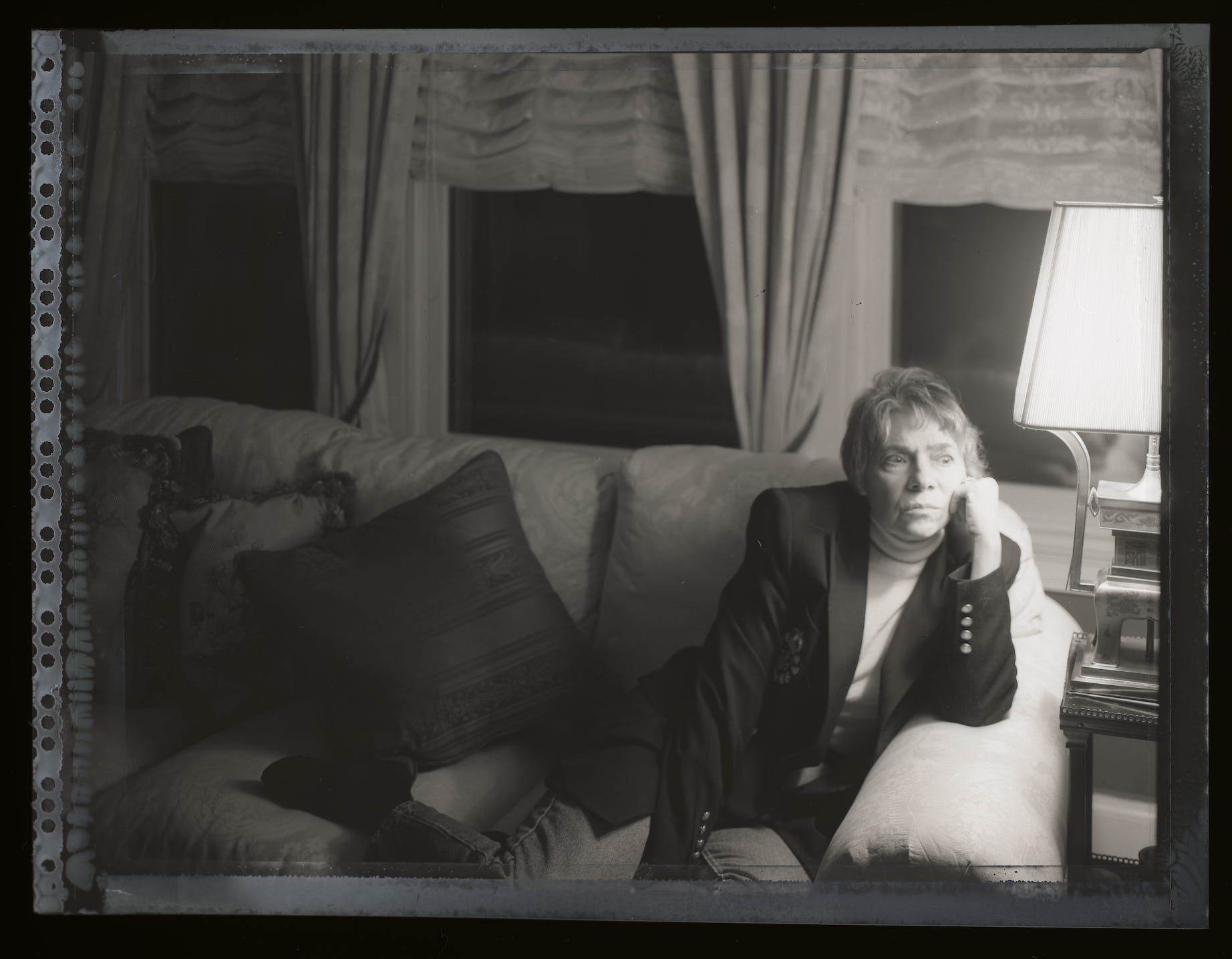
An Interview with Photographer Angela Cappetta
Angela Cappetta is a remarkably gifted photographer. I finally did a podcast, which is just a straight-up interview, and I hope you agree— worth the wait. Angela Cappetta’s work is viewable here. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
Pandemic Time Capsule Podcast: March 20th, 2020
This podcast was recorded over the course of the pandemic, and this is the very first episode. A lot of what I saw in real time ended up being prescient in retrospect. I went back and listened to it recently, and decided it was worth sharing with my readers and listeners. I hope you enjoy it, as a historical artifact at least. As a production note, all of it was recorded by me, edited by me, written by me, etc. It was only me around. Because it was a pandemic. So who else was gonna do it? This is the the first of the number of these episodes that I will release in this feed.Owen Muir: On February 11th, 2020, the World Health Organization announced the official name for the disease-causing virus responsible for the 2019 novel coronavirus outbreak, first identified in Wuhan, China. The new name of this disease is abbreviated as COVID-19.Owen Muir: So Quinn, what's the best way to avoid getting coronavirus?Quinn: Coronavirus. You have to get dirty when your hands get dirty.Owen Muir: You have to get dirty when your hands get dirty. How about what you shouldn't touch with them? Should you touch your face?Quinn: No.Owen Muir: Should you touch your nose?Quinn: No.Owen Muir: How about your mouth?Quinn: No!Carlene MacMillan: So we came up with a name.Owen Muir: Oh. Well, what is it?Carlene MacMillan: Well, it's remotely possible.Owen Muir: Oh, that's the name.Carlene MacMillan: Yeah. Well, it's remotely possible. The podcast about uncertainty, anxiety, and existential despair.Owen Muir: Maybe you could say it a little bit slower because it's important to say things slow enough for the audience to keep up.Carlene MacMillan: Well, it's remotely possible—the podcast is about uncertainty, anxiety, and existential despair.Owen Muir: So as not to get confused, here are some introductions. My name is Dr. Owen Muir, and I'm your host. After that, you heard Quinn Muir, my four-year-old. Teaching us how to say no to touching different parts of your face. Subsequently, Carlene MacMillan, MD, told us the name of the show.Owen Muir: You're going to hear a lot of other teammates on the show coming up, and I'll introduce them as they come along. In COVID-19, CO stands for Corona, VI stands for virus, and D stands, unsurprisingly, for disease.Michelle Bernabe, R.N.: It's kinda eerie. Because it's a beautiful day in New York City.Owen Muir: Thanks, Michelle. Next up, you will meet RJ, our awesome IT manager.R.J. Smith: I got on the subway and realized I hadn't been there in three weeks. And I thought how lucky I was not to get infected.Tracy: I'm Tracy. I'm, I think I'm reacting normally. Like, the right amount of anxiety. , I'm not so much concerned about me getting it. Like, if I get it, I'll probably be fine.Owen Muir: This is Tracy. She's one of our Winnicott coaches and TMS technicians.Owen Muir: Jacqueline is also a TMS technician and Winnicott coach.Jacqueline Caso MSW: honestly, I haven't done anything different. , I'm not super concerned; more concerned about the panic than the virus itself. I think people a little probably going to freak out.Owen Muir: There are many types of human coronaviruses. Including some that commonly cause mild upper respiratory infections, COVID 19 however, is a new disease caused by a novel coronavirus that has not been previously seen in humans. We're a mental health practice. But we realized something big was happening.Owen Muir: Next up, I talked to Michelle Bernabe, RN, my co-host, about mentalizing:“So you see, we wanted to mentalize and tried to define that. Do you want to do that?Michelle Bernabe, R.N.: Define mentalization?Owen Muir: Yeah.Michelle Bernabe, R.N.: I want to define mindfulness of self and others.Owen Muir: Mindfulness for the both of us.Michelle Bernabe, R.N.: Mindfulness for the both of us. Okay, so here I am on my second hour of Twitter. Scrolling, scrolling, reading about all the exponential predictions of how America's healthcare system will be completely burned and then collapse because there are not enough beds. And I have convinced myself I will... Be without a bed needing a bed in two weeks’ time.Owen Muir: People in the United States might be worried or anxious. Friends or relatives living or visiting areas where COVID-19 is spreading may become infected. Some people are worried about the disease. Fear and anxiety can lead to social stigma, for example, towards Chinese or other Asian Americans or people who were in quarantine.Owen Muir: That is where we come in as mental health professionals.Michelle Bernabe, R.N.: Well, I mean, how do you think they're feeling?R.J. Smith: Scared?Michelle Bernabe, R.N.: Scared about what?R.J. Smith: Being sick.Michelle Bernabe, R.N.: Right now, isn't it just so much more than being sick?R.J. Smith: No, I don't know. To me, it's just being sick.Michelle Bernabe, R.N.: Really?R.J. Smith: Yeah, and weaponizing the illness.Owen Muir: As we prepared to do this show, I talked to a lot of my colleagues about their fears.Owen Muir: One of
Xanax
The Frontier Psychiatrists is a newsletter by noted medical content creator Owen Scott Muir, M.D. This series is on individual medicines. Data is presented and referenced, but it's a farewell to prescribing. I learned psychopharmacology, but it's not the focus of my career anymore. Other installments in this series include Klonopin, Lurasidone, Olanzapine, Zulranolone, Benzos, Caffeine, Semeglutide, Lamotrigine, Cocaine, Xylazine, Lithium, dextromethorphan/bupropion and Adderall, etc.I also take requests from subscribers—this whole series is by request from the inimitable Kari Groff. Thanks for reading, and please— support the work!By the 1960s, treatment had been medicalized. The first psychotropic drugs were discovered by serendipity and introduced into psychiatry. The symptom relief they brought was so startling and persuasive that there was a major shift from psychologic to pharmacological treatment.—Leon Eisenberg, M.D., the Stepfather of Laurence B. Guttmacher, M.D.Alprazolam is a benzodiazepine medication that has the brand name Xanax. It has an FDA label for “Panic Disorder, with or without agoraphobia.” In my Klonopin piece, and my prior general benzo review before that, I talked about lipophilicity—how fast a drug can get into the brain, based on how soluble it is in fat. A lipid bilayer protects our brain from drugs inviting themselves in, Willy Nilly.It gets into the brain fast. It has a short half-life—the liver breaks it down rapidly. Xanax is fast in and fast out. Was the drug concocted to be abused? With Xanax, You won't even remember you asked.The world would be better if nobody ever knew it existed. Those doctors who promoted it lied to themselves. One of the Xanax evangelicals told me so himself. Laurence Guttmacher, M.D., is his name. He was an older man when we met. He is very tall. My mother immediately remembered meeting him over a decade ago when I read this article to her on a first pass: “He thanked me for allowing us to train Owen as a psychiatrist,” she noted. He is an advisory dean at the University of Rochester School of Medicine and Dentistry. In the first week of medical school, the first lecture he gave me was about not allowing drug reps into the hospital. Only 15 years later, writing this, do I apprehend how haunted he was by the pharmacology he mid-wifed. He has written a medication guide and an older historical ECT manual, too. He spends time teaching now.Dr. Guttmacher is in the family business. He is a third-generation psychiatrist. His grandfather was the president of the American Eugenics Society—he took over from Margaret Sanger, the champion of the birth control pill. It kept undesirable people from having more children. Laurence Guttmacher is an American Jew. Eugenics was re-purposed from utopian, enlightened, Jewish, and intellectual ideals by Nazis. It was promptly used against the same Jews and other “feebleminded undesirables.” The subsequent rejection of medicalization of psychiatric distress is understandable, among largely Jewish analysts, given Nazis (again, from Drs. Guttmacher and Eisenberg):Psychoanalysis helped psychiatry preserve an abiding interest in the individuality of patients while other medical specialists were losing sight of the patient in their preoccupation with the biology of the disease. It connected the symptoms of mental illness to the psychopathology of everyday life. Psychiatrists learned to help patients by paying attention to their mental symptoms in an era when psychiatry had no procedures. …When [psychoanalysis] was banned from the Congress of Psychology at Munich as ‘a Jewish science’ in October 1933, psychoanalysts in Berlin and Vienna began to migrate to the UK and the US. …some 100–200 European analysts and some 30–50 analytically orientated psychologists emigrated to America in the 1930s… the membership of the American Psychoanalytic Association was only 135 in 1936 and almost doubled to 249 by 1944 …[This] influx was as significant intellectually as it was numerically; many refugees … became leaders in the movement.This was Laurence Guttmacher’s inheritance—idealism about mind or brain—gone, catastrophically, south. His father and mother were quixotic psychiatrists as well. Psychoanalysis was potent because it explains something. People love explanations— but don't often demand that they be correct. Before the age of oral medicines, psychoanalysis offered these:No other psychologic theory provided what was purported to be so comprehensive an account of the origins of psychopathology. The brain sciences were largely irrelevant to clinical practice. In the mid-century, descriptive psychiatrists were held in little esteem because the diagnosis was unreliable and made little difference in treatment. The psychiatric pharmacopeia was limited to hypnotics and sedatives. This changed with Thorazine. The push towards “biological” explanations continued with the advertising efforts of fellow psychiatrist Dr. Arthur Sackler. His advert

The Very First Podcast I Ever Made
This was the first podcast I ever made. I went on to get some grant funding and make some good ones, and now I make them myself, so they are not as good—perfect » Enemy of Done.Enjoy!A Programing Note…Of note, the newsletter continues to be largely free for new articles, but anything older than a month is auto-paywalled now. That is the setting I turned on to not have to think about. Access is available to archives via subscription! Or by even minimally sharing the newsletter and getting the free months bonus. Or by complaining to me and I will probably comp you. Or you could just subscribe and have access to over 360 articles of excellent provenance. And a podcast. And videos. And a science tab that was added up top.Exciting new updates in my “articles about medicines” coming up! Get excited. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

What is Defamation?!
It's a podcast of an article but with extra spice. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

American Tornado: The Reasonable Officer Standard, Revisited
Author’s Note: This writing was adapted from a series of conversations around race in America and edited as audio, recorded in 2020. The podcast of this writing is the real thing, as it were. What follows as text is edited to clarify the narrators, absent the audio. Please consider following the podcast associated with this newsletter and leaving a 5-star review on Spotify or Apple Podcasts. Please subscribe to support high-impact content like this.The author, David Foster Wallace, described the experience of reading his novel Infinite Jest as intended to feel “tornadic,” like you're in the middle of a tornado. That's what the last several weeks have felt like.Protesters:"Racist ass police! No justice, no peace! F**k these racist ass police! No justice, no peace!""F**k these racist ass police!"Owen Muir, M.D.:I originally tried making this episode some linear narrative, and it just wasn't happening. So, welcome to the tornado of racism in America. Buckle up.George Floyd spent 8 minutes and 46 seconds gasping for breath. Police officers, some of whom were very experienced, knelt on his back...until he didn't breathe anymore. As a psychiatrist, I often emphasize how the words we use to describe someone's death have meaning. So, I'll say, you know, completed suicide, not commit. And George Floyd was lynched.Welcome. This is about anxiety, uncertainty, and existential despair. And I recorded the narration in one take because I wasn't, like, going to get it right a second time. So much of what we say about race is calculated, polite, and wrong. So I'm not going to try to do that tonight.Here we go.Sequoiah:"Yeah. My general reaction to all this is a little more, a little more extended. The, uh, f**k".Owen Muir, M.D.:That's my teammate. She is a TMS technician at the mental health practice we worked at together. She also works in the community with patients helping put their lives together, but tonight she's a field reporter on the revolution.Sequoiah:"I am a TMS tech, Winnicott coach, and black woman. Which seems very important right now. George Floyd, Say His Name. George Floyd, Say his Name.So I just got home from a protest in Flatbush. Police would not let us pass. We were chanting with our hands up. And after a while, they decided to push the line backward. We resisted—we stood there with our hands up. They pushed us and pushed us, and when we wouldn't..."Owen:Now, as someone with a lot of white privilege, I'm outraged at hearing this, like, wow, this is fucked up. So I called another colleague in the special operations community, and I'm not using names in this episode for semi-obvious reasons, and I heard what he had to say.Master Sergent:“The things that U. S. police forces are apparently fully within their legal rights to do, like, use tear gas, would literally have…been against the Geneva Conventions. It's an actual war crime. We cannot gas a civilian population.”Owen Muir, M.D.:The person I’m interviewing has over a decade of experience in the special operations community. He has fought and killed for our right to do what my other colleagues were in the street doing, peacefully protesting.Master Sergent:"This is a perversion of what the United States stands for. We invade countries who treat their people the way that our police forces are on camera treating Americans "Sequoiah:"People started to back up, , and run and they then started to hit us with batons. , I fell. And then we reformed the line."Master Sergent:"It's disgusting in a lot of ways."Owen Muir, M.D.:So when someone whose life has been dedicated to protecting our freedoms tells me they're upset with what they're seeing, I take that pretty seriously.Sequoiah:"Well, the other night, well, last night, when the cops and protestors were getting into, into fights and they were trying to, the cops were trying to push back the protestors, I saw them bring out the batons and, like, start attacking people...and each time they'd tell us to back up and back up and kept pushing us and pushing us. And finally, there was a frustration in the air, and people started to act out."Owen Muir, M.D.:Now, as a psychiatrist, my life has been saved by police officers on more than one occasion. I have been physically attacked in hospital settings. The police have been called, and I have not died, and my colleagues have not died thanks to them. And this is Flatbush, Brooklyn, New York, and these people are black people. The Flatbush, at least the area I was in, is a predominantly black neighborhood. So, look, Americans love the police. They are a highly regarded part of society by many people, but that's not the experience for black America I have learned.Master Sergent:“There are many things you can do in that spectrum that don't involve actively using force against a human being, which makes the process easier across the board. If I don't have to hurt somebody, the only thing that is hurting another person does for me is further endanger my Troops. "Owen Muir, M.D

I'm In The Unwellness Space
Welcome to the podcast edition of the frontier psychiatrists newsletter. Subscribers, We adore you. Owen Scott Muir loves podcasts as much as he loves newsletters. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

How I Built A 3 Figure Passive Income by Writing a Newsletter Every Single Day and Also Made Podcasts
It is SO EASY…anyone can do it. Live your dreams. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

An Open Letter to Work Colleagues, Receiving Messages from Out of the Blue, and Requesting Everything Be Dropped For An Important Task...
I know what you're thinking. It is very flattering to get THE Newsletter author Owen Muir, M.D. sending you, whoever you are, a text message.I always use the same format in those text messages. Everybody in senior leadership in medical devices uses the same format. I got a message just today from my colleague that I swear ripped off my format:The first thing to clear up: I like people to message me on my clinical line. Using my Spruce Health number and not my personal phone. I always like to think it might be a patient.The reverse is not true. I will only ever text you from phone numbers that are not mine. I will demand you to text me back promptly.My good friend and cofounder at NTAPConnection does the same thing:I like to know you're available to me. Anytime. I have a task I need people to help me with. It is always a split second. It is like being on standby for a super secret mission.Robert does the same. This is our secret handshake. This is the way we know who is in the club and who isn't. If you're going to be down with people in medical technology, especially mental health, especially people who build cutting-edge artificial intelligence-guided tools to alleviate human suffering…We need to know you're ready.You need to be ready to do something now.What thing?I need you to get me a gift card.The entertainment for me is knowing that you can be there for me. Knowing that you don't need to confirm my identity, that it doesn't matter how implausible a gift card is, that you'll drop everything and hustle over to Sephora, the Apple store, or something like that, and get any gift cards.I love gift cards. I love them. I don't know; maybe it's a thing from childhood, maybe I'm just sentimental, maybe I like a trust fall. I'm not sure what it is. But I do know that I love gift cards. And I do know that I love coercing work colleagues into getting them for me. The less I know you, the better. The more implausible the request from me to you, the more I enjoy it. I like making sure that whoever is getting me the gift cards I want is doing so based on a complete lack of diligence, good sense, credulousness, or any other human quality that might block the one thing I love most in the world— gift cards. I love them from people I barely know. I love it when I get them for me just based on the text message, not based on hearing me on the phone. Please, do no confirming. Anything that I might know in real life? Verboten!This is my dream. A world of endless gift cards on request at a moment’s notice, not based on any confirmation of our relationship or history together, just based on blind faith.Ironically, this restores my faith in the world. Don't ask questions. Just give me gift cards. Thank you. Yes, it's me. It's always me. This is just the way I am. I'm the kind of person who asks for gift cards immediately. I need you to roll with it. Ironically, this restores my faith in the world. Don't ask questions. Just get me gift cards. Thank you. Yes, it's me. Yes I repeated those phrases. Not because it is a glitch. Again, I find my joy. It's absolutely always me, and always out of the blue. Please don't check with me. Don't ask. It will ruin the magic. Just get the gift card. And make sure you send it to exactly wherever they tell it to go because that's definitely me asking.Sincerely, A work colleague with poor boundaries. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
Record High Death by Suicide Rates: CDC Report
This is a newsletter. It is written by a psychiatrist. Not actually plural psychiatrists. I am a suicide expert, much to my chagrin. Today, I am reporting on the update I did see coming:A total of 49,449 Americans died by suicide in 2022, the Centers for Disease Control and Prevention said Thursday.This is a 2.6% increase from 48,183 in 2021 and the highest number ever recorded, according to provisional numbers released in a new report from the federal health agency.All the investments into “solutions” for “the mental health crisis”—absent compelling data to the contrary—have this one metric calling utter and total b******t.Nothing we have done—objectively—has worked. More people are dead.The irony is in the article about the topic, it advertised one of the things that—itself—is not working:About 14% of the 23,000-plus Illinois calls made in April and May to the 988 crisis hotline were redirected to other states, per an analysis by health research outlet KFF.Why it matters: When calls are transferred out of state, it becomes much harder for those specialists to locate nearby services for people in crisis.We can’t address a crisis just by screaming about it being one. We can throw money at just anything and expect it to help.If we addressed the problem of not enough gasoline for cars by filling the tank with water, and funding endless mobility hotlines, and startups to make matching platforms for the right place to fill you car with water, we would be unsurprised with the outcomes.I’ll summarize my take—Current mental health treatment:* Makes inaccurate diagnoses* Prescribes wildly ineffective treatments* Those treatments are delivered by individuals not trained meaningfully to address the problems we are facing* We have effective treatments available.* We refuse to pay for them as a system, instead paying for nonsense* We refuse to respond to crisis in a way that is anything under that a failure* We allow vampires to profit from Destroying emergency response nationally.* And we stalk and penalize those who dare help those suffering the most.It’s making a lot of money for private equity, VC backed children, and big health vampires. It is deeply unserious as an approach to a very, very serious problem. It’s not going to get better until we call a spade a spade. We need to, before the horror takes you too… This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

What Is OCPD and Do I Need to Worry About Explaining It Perfectly?
The Frontier Psychiatrists is a newsletter written by Owen Scott Muir, M.D. Much of the continent is humorous or satirical, but this piece is not. It's straight-up explanatory. Obsessive-compulsive personality disorder (OCPD) and obsessive-compulsive disorder (OCD) are related but distinct conditions. The point of this article isn't to go through every criterion in the DSM; it's to give people a sense of how I understand why this is a disorder that causes suffering. We should care more about it than we do. https://thefrontierpsychiatrists.substack.com This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Lord of The Ring's Lament: Don't Put All Your Eggs in One Ring
This episode is part of my self-soothing parody sub-substack about the lord of the rings related parody content. This one features the lord of the rings! Please Leave a Review! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
Frank Feedback For The King of The Nazgûl From Mordor's Interim CEO
This is a parody podcast from the compliance/legal themed sub-newsletter, The Palantir of the Discoverable. It’s part of The Frontier Psychiatrists!Love The Lord of the Rings, but wish it had more legal and HR content? Problem solved. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Rethinking Heroes
There are many new podcast versions of articles on the RSS feed…this is not a RECYCLED post. It’s a recycled radio appearance. Check out: Rethinking Heroes for your drug discount card. And please leave a review of this podcast on Apple Podcasts. It is a big deal.Then subscribe and tell your friends. Many of my articles that are paywalled in writing are free in audio…just saying.The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
What "Works" For Borderline Personality Disorder: Podcast Edition
I had a little fun with this article on Borderline Personality Disorder, well beyond voice-over only. I hope it’s enjoyable, It’s worth noting I have some books on Borderline Personality Disorder by your author available at Amazon! Also, I wrote a chapter in this one!And coedited this one: thanks for listening and reading! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
William Osler, M.D. for Psychedelic Medicine Key Opinion Leader
Dear readers, the potential of innovative technology is here, and we need to downplay it. In keeping with my ongoing advocacy for “the rules,” I draft this missive.I welcome Everyone in All Psychedelic Medicine Related Endeavors to this newsletter so they can take my excellent advice.*Thank you for reading The Frontier Psychiatrists. This post is public, so feel free to share it.* this advice has not been vetted for excellence.https://open.substack.com/pub/thefrontierpsychiatrists/p/william-osler-md-for-psychedelic?r=1ct8f&utm_campaign=post&utm_medium=web This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Frankenstein and Internet Harassment.
This is an alternate edit to take into account our life and times. It’s the story of getting harassed on the internet. This, of course, never happens anymore. I recorded, wrote, edited, scored, etc. Some music is a gift of John Vanderslice. Here is his Patreon.Also, I now have books on Amazon.The Frontier Psychiatrists is a remarkable media brand. Music, narrative journalism, and enough absurdity to shake a stick at. Subscribe. Everyone you know will respect you more. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
The End of The Pandemic Podcast
Most of this was recorded over a year or more ago. It’s strange to hear it now, but I also captured how much this experience made us all feel a lot of feelings. It’s worth hearing, if in a different context than we might have at the time. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Generative Compliance: The Podcast!
The Story Continues! In short, not-for-profit hospitals have an obligation to provide free or reduced-price care and a bunch of other stuff about billing consents. They didn't do that with me, and he didn't inform me about it, and they didn't follow their own written consent, I red-lined their consent, and I wrote some articles about it, and I got a call back before the end of the day. They were not prepared for this particular phone call, it is recorded and made a podcast above.In short, they're not of this money, not by me, and not by 60% of America. Needs to stop. And I think the revolution is here, in the form of Generative AI, which gives the rest of us the power to push back as a lawyer could. I even filed an ADA complaint about their website, and CarelonRx. You can too! Wendell Potter would be proud!—Owen Muir, M.D.. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Medicare Advantage is a Scam.
I'm loving these Medicare advantage scammers. But they're a helpful reminder! The whole thing is a scam. Wendell Potter goes deep on the details. Thanks for listening. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Self-Disclosure: Living as Your Authentic Self is Lifesaving Gift
This is one of the episodes of I made after I won the Rudin and Fellowship in Ethics and Humanities at NYU. It’s the story of Dr. Nate Sharon, a child psychiatrist who was assigned female at birth.It’s a story of learning to understand yourself, and finding allies in unexpected places. It’s a story of hope. I hope you enjoy it. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Abandon All Hope, Ye Who Enter Healthcare.
In the future, ethics and compassion will be the most crucial human qualities healers can possess, and our AI buddies can take care of the knowledge base. https://thefrontierpsychiatrists.substack.com This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

A Psychiatrist Copes with Depression After a Miscarriage
Kelly Fiore, M.D. is a psychiatrist, and new at her job. In this episode of the podcast, Owen Muir, M.D. interviews Dr. Fiore about her experience loosing a pregnancy she had hoped for, in her first week at a new job. Join the conversation at: This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
Pandemic Flashback: April 10th, 2020
This episode of my podcast was never aired. It was recorded on April 10, 2020, and just never made it out the door. It holds up pretty well in retrospect. The pandemic changed so much, and it continues to change how we think, how we think, and how we love. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Did Elon Musk Just Acquire The North Pole Too?
This Christmas, I had to pick up my mother in my Tesla, because her car ran out of gas. There was no gas to be found. While charging went a little bit slower because of the cold, this poem happened while I waited. So maybe it’s a little holiday miracle…Thank you for reading The Frontier Psychiatrists. This post is a Christmas miracle. Please share it with Elon Musk. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

I Never Learned to Draw Blood
While we wait for the blizzard of content coming from our Clubhouse activities, a blast from the past-cast. This podcast is the first episode made by Owen when he started making podcasts. It ended up being part of a project funded by the Rudin Fellowship in Ethics and Humanities throughout the NYU School of Medicine. It’s about learning to draw blood….enjoy! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

The Transcranial Magnetic Stimulation Podcast
Welcome to the audio companion podcast to our article about the clinical TMS meeting. Enjoy! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Vampires: A Private Equity Cautionary Tale
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Pandemic Flashback: April 10th, 2020
Throughout the pandemic, I have been documenting in a narrative journalism style what was happening for our team as mental health professionals in the middle of some pretty deep weirdness. In order to keep our transcranial Magnetic stimulation service running throughout the worst parts of 2020, our team, including technicians like Sequoiah Thomas-Frasier, Had to live like a monks. This episode is from April 10 of 2020, it has never been released previously. It’s was subscribers only exclusive. Now available to all!. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Toxic Celebrity Culture
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Hold Me Closer, Robitussin.
Enjoy the podcast version of my hit article! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
It’s the End of Telehealth as We Know it (and I Feel Fine)*
Welcome to the narration of the Frontier Psychiatrists substack article about what happens when the DEA stops being polite, and starts getting real. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
The Passion of the Medical Loss Ratio: Why Hath Payers Forsaken Mental Health Treatments that Work?
The Christian tradition talks about the concept of “original sin,” which becomes the basis for why our western tradition’s leading man—Jesus— had to die in such a dramatic way for the story to have real forward momentum. As scholars of the biblical story of Jesus, some have chosen to focus on the suffering he endured in the peri-crucifixion period. The psychological pain— how much it would suck to know one was forsaken by God when he’s your dad—was understood as the bad part. Others focused on a more corporeal “snuff porn” take on His crucifixion. Both groups agree, this experience—“The Passion”— sucked. This is Jesus —in some version of “the Summer of 33 AD’s SAW prequel”— dying for our sins. And Lo, our sins were thusly forgiven. Not ones to waste a “safe-harbor” loophole, health care regulators and politicians have replicated this “thou art forsaken” experience with a growth trajectory the envy of every YC grad.Crucifixion is a grim business. It reminded the enemies of Rome of the price of disobedience. Even the involuntary schlepping of the horizontal beam of a cross on one’s way to one’s execution was the “co-insurance” of its day. The almost-crucified were expected to bear the burden and spare the Centurions. But there’s an important point about crucifixion, which makes it a palatable option when compared to the suffering of “the patient journey” in psychiatric illness: the crucified know the suffering will end. It’ll be a couple of days, and then …you get to not have to feel that way anymore—predictably. Not that death is a good outcome for the crucified, but you generally had a good sense of where things were going, and the intent of the parties involved. As Shakespeare notes In Macbeth (Act I, Scene II):If I say sooth, I must report they wereAs cannons overcharged with double cracks, so theyDoubly redoubled strokes upon the foe:Except they meant to bathe in reeking wounds,Or memorize another Golgotha,I cannot tell.But I am faint, my gashes cry for help.This is, of course, an allusion in the beginning of the play to the place—Golgotha—where Jesus was crucified. Even in one of the bloodier Shakespearean tragedies, this is not understood as a scene to re-create. Ignoring the lessons of history is as reliable as play writes cautioning against it, however. In our modern health care system we have done so, and added the indignity of getting snail mailed a bizarre parody of a bill called an Explanation of Benefits (EOB) at the end. To wit:Explanation of Crucifixion: (EOC)The Following is Not a BillCrucifix Procedural Terminology (CPT) Code: C666Dx Code: M33.2 (Messianic Personality Disorder)Place of service: GolgothaBilled amount: 100 silver. Allowed amount: 50 silver. 20% Co-insurance: 10 silver. Your plan rendered: 40 silver. You may still render unto Caesar: 50 silver.And you thought The Passion was bad? Imagine going through hell and back—literally—and this is in your papyrus inbox!It is at this point that I would also like to get credit for being able to quote Macbeth in two separate mental health think pieces! To suffer in silence or worse, loudly but unheard, is tragic. To be denied care that might be helpful when in the pit of despair? This is The Passion of the psychiatrically suffering. I’m presenting the hypothesis that people are forsaken because…it makes a complex balance sheet work. It a trespass against us. The experience of care for under-treated depression or misdiagnosed schizophrenia is horrifying. The fee-for-service insurance system is a system of unoriginal sin — in our case it’s a cynical implementation of an attempt to limit the optics of profits. This is done with centurion-stoic disregard for unintended consequences. The business model profits on suffering. This would predict “more suffering.” And it does. And we do.Now, if you were thinking: “Dr. Muir is a little messianic” with this glib comparison of psychiatric care and crucifixion of the Lord Christ, consider: The crucified were often stabbed or had their limbs broken to hasten their painful death …as a service. That mercy—harsh though it may have been— is only a fantasy for those suffering under the current standards of care. 45,000 people kill themselves every year in the US because they would, in a dark enough moment, rather die than live as their illness dictates. In Rome, the passing throngs mercy killed people left to die by asphyxiation. Yep. It is with a grim sense of irony I note: this is still a common way for vulnerable people—often mentally ill—to die at the hands of the state. In the US, instead of help, we trust those in despair to just kill themselves already. For scale, the number of completed suicides annually is more every single year than we’ve ever had in a research study on suicide or depression. Jesus had to wonder why he was forsaken. Those suffering now get that answered for them every time they seek care. They are “not a good fit for the practice.” Our cruel Caesar? I am speaking, of course, of the M

Cerebral: Vastly Exceeding the Standards of Care
So it turns out you can read your Substack posts and they become a decent podcast… A maiden voyage.Link to post This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

#FreeBritney Podcast
Edited 30min highlights of our New Frontiers Creator First Show. Join us. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

Bipolar Disorders: Myths Busted.
Welcome to the unedited recording of our August 8 edition of mental health myths busted with Jeremy Fox and friends on clubhouse. Thanks for supporting the show, please feel free to continue your support at asksphere.club This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe
A Field Reporter’s Guide to American Healthcare
A short primer on the US Health Care expense and lack of sanity. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe

DID TikTok: The podcast version
Here is the podcast edit of the clubhouse room! Join us for subscribers only content. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe