
Sensible Medicine
131 episodes — Page 2 of 3

Ask me anything
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 45: Patients
The woman with palpitations.The man with whom you used to joke and trade barbs who now sits silently, absent, while you talk to his wife.The woman whose depression dominates every visit; her depression being the one problem she refuses to address.The man whose joy and charisma makes every visit an absolute pleasure, despite his painful disability about which you can really do nothing.The man who never complains. Well, not never. The two times he did complain he ended up with emergent bypass surgery and a diagnosis of acute myeloid leukemia.The woman whose concerns are always uninterpretable. You wonder if the problem is your lack of cultural competence, that her language skills prevent her from articulating her problem, or maybe that her ineloquence keeps her from even knowing what she is experiencing.The woman who asks how you are doing because she recognizes that caring for her, with her dreadful prognosis, is hard.The man who, forever unsatisfied with his health, never accepts your advice, dismisses consultants, yet never misses a visit, praises you as the greatest doctor, and brags about you to his friends.The man whose world is spinning.The healthy 27 year old who is sure that her tension headaches are from a brain tumor.The man who berates the front desk staff, makes inappropriate remarks to the medical assistant, and has made racist comments to your nurse, but in the exam room – alone with you -- is the perfect gentleman.The man who laughs when you pull down his sock to examine his edema and a wad of cash and a dime bag of cocaine fall on the floor.The 75-year-old daughter who accompanies her 95-year-old mother to visits. You know that the older woman’s death will liberate and devastate the younger woman.The man who always exaggerates his symptoms because he is terrified by his own mortality and worries that he won’t be taken seriously.The woman who seemed impossible when you first met her but now brings you joy when the urgent care doctor calls and asks, “How have you taken care of this lady for 15 years?”The woman who doesn’t seem to like you and never seems to trust your opinion but, after 20 years, refers her daughter to you.The woman with six years of dyspnea and no diagnosis.The man you agree to see after he was “fired” by a colleague. His care, and your relationship with him, become an inspiring, and even rewarding challenge. He fires you after a year.The woman whose relapses, lies, and prescription forgeries angered and exhausted you for a decade now sits in a wheelchair, caregiver by her side, vacant.The woman who comes to see you for a new patient visit because her husband, your former patient, insisted that she start seeing you after he died.The man who hanged himself three weeks after he saw you. He had complained of fatigue.The man who apologizes because he sees it has been difficult for you to give him the news about his recent scan.The woman with painless jaundice.The patient who fires you, deservedly, because you made a rookie mistake.The man who brightens your day when you see him on the schedule but honestly, if you didn’t know him, you would probably move to the next train car if he got on.The patient you secretly hoped would change doctors and then, when she does, you feel bad that you failed her.The man who steps off the scale, places a thick wallet, two rings of keys, and a Glock on the exam table before getting back on the scale.The man who wrote a thank you note that he had his wife mail to you after his death.The man who fought you until the end, always wanting more treatment, even after every doctor told him we had nothing left to offer.The woman whose diagnosis you could never make, until you got a pretty good idea of it ten years after she died.The man who just has a cold. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Sensible medicine ask us anything part 2
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Ask us anything podcast
This podcast is one of three we will be posting to answer the questions that came to us in response to this post. We had a nice set of questions so we will certainly be doing it again. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Back to Sleep Series in Audio Format
I learned a lot from Elizabeth Fama’s multipart series on the back-to-sleep recommendation for infants. She agreed to put the entire series into an audio file. Here you go. JMM Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 44: Diagnostic Enigma
Ask general internists what they love about their field, and they are likely to talk about long-term relationships with patients and the pleasure of solving clinical puzzles. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

How can we do better as a county hospital?
My lecture to the cancer care staff at a county hospital. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 43: The Absence of Reassuring Counterfactuals in Clinical Medicine
Even when a decision is clear, and things turn out badly, the lack of a counterfactual allows endless second guessing. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

What Medical School Looks For and What Medical School Should Look For
I discuss how medical students are selected, and perhaps how they should be selected. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

The Retirement of Dr. Mark Siegler
Remarks about a model clinician. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 42: Patient Approaches to a Doctor’s Visit
It would be foolish to argue that doctors are unaffected by how they are treated by patients. Their treatment may not affect the care they deliver and only affect how they feel at the end of the day. It is probably impossible to know. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe
A Discussion with Professor Venk Murthy on Coronary Artery Disease
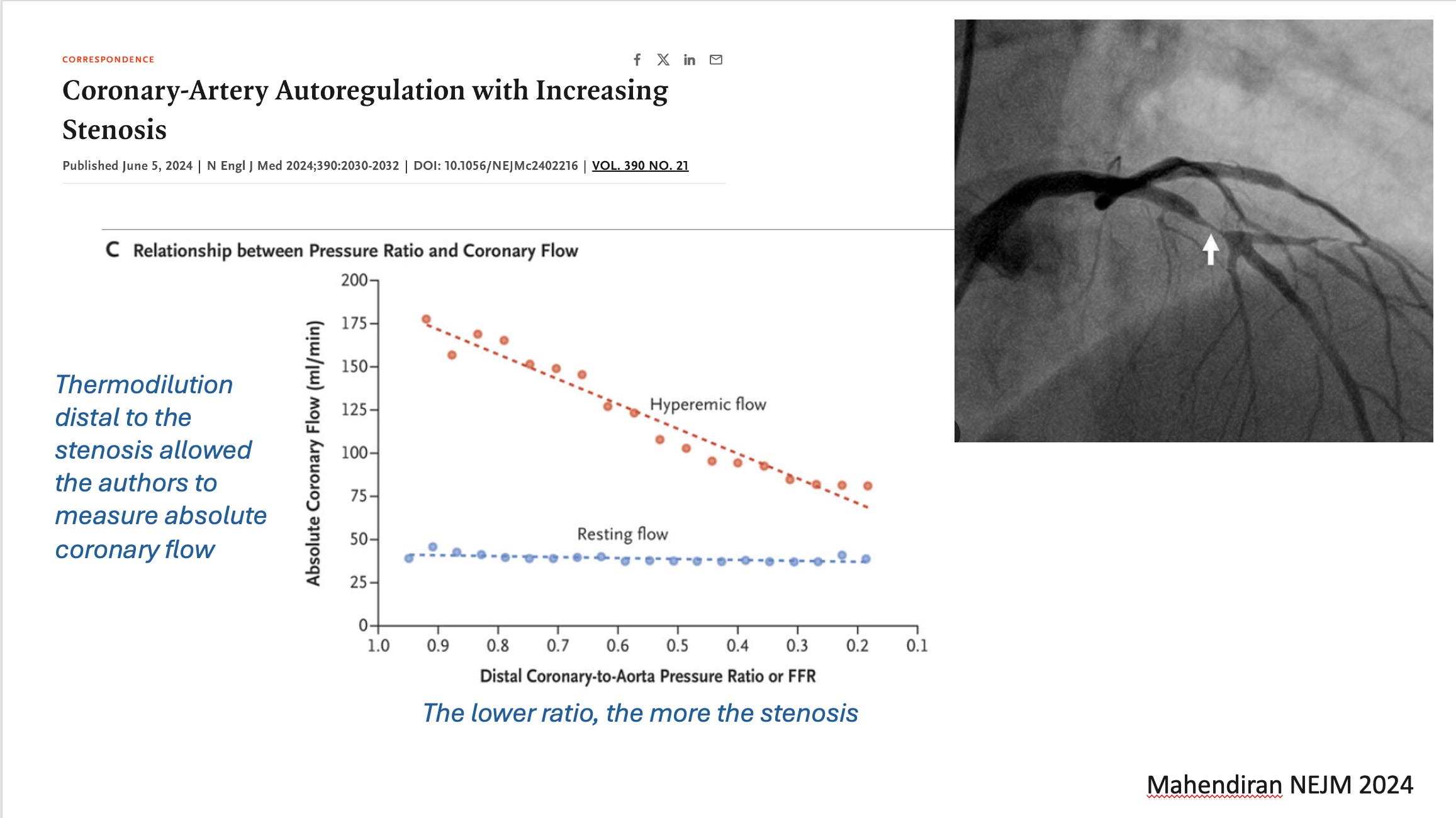
When I type the words coronary artery disease I bet that you picture angiograms with stenotic lesions—blockages in colloquial language. Indeed a high grade plaque from atherosclerosis in the inside of a coronary artery can limit flow to the heart muscle. But. But. Not as much as you think. You know why? Because there is something called the coronary microcirculation. Before blood gets to the beating heart muscle it has to go through small blood vessels. So small that you can’t see them. A study in the NEJM—on one patient—elegantly shows the ability of the microcirculation to autoregulate blood flow in the face of increasing degrees of obstruction in large coronary vessels. We’ve all seen patients who have severe flow-limiting proximal stenoses, which create little to no angina. A likely reason is the ability of the microcirculation to dilate and improve blood flow—at least at rest or minimal exertion. My friend Venk Murthy explains this elegant study. I learned a bunch and likely you will too. We refer often to this figure from the paper. It would be useful to have it handy while you listen. JMMRemember all, Sensible Medicine is a reader supported site that is free from industry advertisement. Thank you for your support. Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Impella, Mammograms and Med School Fails Students
VP fixed the audio This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Fear and Opioids in Academic Medicine
Regard for power implies disregard for those without power; part 3 This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

A discussion with interventional cardiologist Dr David Cohen on medical evidence, TAVR and stroke prevention
David Cohen is one of the smartest docs on Twitter. I learned a bunch talking with him. The procedure called transcatheter aortic valve implantation or TAVR is a damn miracle. In days of old, a heart surgeon would have to saw open the chest and cut out the heavily calcified immobile aortic valve and sew in a new one. I watched a case as a young doctor and came away shocked that patients survive this surgery. TAVR is even more stunning. Doctors place a valve up the aorta, across the diseased valve, and then place the new valve into the old valve. The verbs squishing or smooshing come to mind. The other unbelievable thing about TAVR is that strokes are less common than you’d think. When I first heard about TAVR, I thought: how is it not limited by all that debris going into the brain? Well, there is less debris than I would have thought. But not zero debris. In fact, there is one device on the market that forms a barrier between the aorta and the brain. We call it an embolic protection device (EPD) or cerebral embolic protection (CEP).Early studies show that the device catches debris that would have occluded blood vessels in the brain—iow, caused stroke. The pictures almost sell the device—because, obviously, catching debris has to be beneficial. But. But. There are always ‘but’s’ in Medicine. The PROTECTED TAVR trial, which compared TAVR with and without an embolic protection device failed to show a statistically significant reduction in stroke. It was a good trial, but it did not close the door for the device. For two reasons: one was that the trial was underpowered. The lower bound of the 95% confidence interval allowed for a 1.7% lower rate of stroke in the treatment arm. Neurologists feel that a 1% risk reduction in stroke is clinically important. The other reason was that a secondary endpoint of “disabling” stroke was 60% lower with the device. We needed more data. Another trial is not likely going to happen. Trials are expensive and take a long time. This is where Dr Cohen’s group comes in. They performed an observational study looking at more than 400k patients in a TAVR registry. About 13% got the device and 87% did not. This is where Sensible Medicine readers should start feeling a rash. Why? Because you know how scary it is to try and compare outcomes in two groups of patients who were not randomized. Cohen, however, tells me about a super-interesting way to approximate randomization in this comparison. It’s called an instrumental variable analysis. He explains this to me in clear terms during our conversation. I love methods so I was enthralled. But that isn’t all. The other thing is that his study, like the PROTECTED TAVR trial, came up with tantalizing close results. We discuss that as well. I loved our talk. If you like evidence, methods, and great medical stories, I think you will also like this conversation. JMMIt’s free to all. We appreciate your support for this experiment in bringing ad-free medical information to the public. Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Adam and I discuss the week's medical news
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Cifu, Prasad, Mandrola
A spirited discussion of craziness in medicine This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection #39: What to Expect When You Are Aging
MM is 94 years old. Her only active medical issues are hypertension and vitamin D deficiency. She takes only 20 mg of lisinopril and 1000 units of vitamin D3 each day. She has no cognitive decline and gardens every day if the Chicago weather allows. Her Friday afternoon appointment is the doctor’s last of the week.Sensible Medicine is a reader-supported publication. If you appreciate our work, consider becoming a free or paid subscriber.I’ve already written a reflection on four things patients have taught me. After MM’s visit, I realized how much more there is to write on the topic. So here is a follow up with the unoriginal claim that the most valuable things I have learned from my patients are not about the practice of medicine. Though not profound, the lessons are universal. The longer I practice, and the older my patients get, the more frequently these truths are spoken.Aging is PainfulAnybody who gets to middle age knows that things don’t work like they used to. Around my house we say that any day that nothing hurts is remarkable. My patients are full of pithy phrases to make the point that aging is physically difficult.“Getting old is hard, but it beats the alternative.”“Aging is not for wimps.”“Every time I look in the mirror, I ask myself, how the hell did that happen?”People respond to their progressive disability in all manners. Some fight at every turn. Every visit, irrespective of age, is spent discussing aches, pains, and things that can no longer be accomplished. There are demands for me to make things better. I find it challenging to address the concerns, rather than dismissing them with “it’s just age,” while also letting people know that some suffering is “part of the human condition.”Other people accept frighteningly steep and acute declines. My challenge at these visits is to balance, “She’s not asking me to address the problem, so who am I to pry” with “This actually seems like something I should explore, even if she is willing to accept it.”Where there is little diversity is our ability to adjust to disability. I was taught that people rate the quality of life with a disability higher when they are living with it than when they are watching other people live with it. Thirty years of clinical experience has made this real. We should add to the saying, “There but by the grace of God go I” the addendum “but, when I end up there, I’ll be OK.” Aging is SadWhen I was an intern, I admitted an elderly woman with pneumonia. Her biggest problem was not the pneumococcus but her depression. Her mood made her miserable and the associated psychomotor retardation was going to make her post-hospital rehabilitation impossible. She was already taking an SSRI and seeing a therapist. I called her primary care doctor, a geriatrician. Like a true intern, I expected he would have an answer to her misery. His response was, “Yup, it is a sad time of life.”There is a lot to be said for the golden years: retirement, family, friends, greater financial security – but as the years go on, the psychological costs mount. Besides the physical decline, there is the constant loss. I repeatedly hear, “Everyone around me is dying.” Siblings, cousins, friends. It sometimes seems like those who are most connected suffer the most – that big family that has always provided support now provides an unending procession of funerals.People mourn their losses as well as their own mortality. You cannot ignore what is to come when your peers are dying. Those who deal with this best seem to be the people who can be honest that their grief about the loss of a friend is partly the fear and sadness that they are next.Loss is Never EasyI never felt like I had enough time with MM. Not that she needed time for me to attend to her medical problems. She was blessed with enviable genes and an outlook that combined cheer and steel. I just wanted time to hear more about her life and her experiences. I wanted to learn from her.On one unpressured Friday afternoon we chatted. I did not have another patient to see, another note to write, or another meeting to run to. Her daughter would not pick her up until 6:00 PM. I told her that I still thought about her husband, also a patient of mine, who had died about a decade earlier.She paused and then remarked. “We lived together in the same old house for more than 60 years. Every time something stops working there, I curse the damn house and I curse Charles for leaving me alone in it. He was always puttering around, fixing things. Then, of course, I think of the wonderful years we had here. I cry because I still miss him, and then I thank the house for reminding me of him.”I can’t write anything original about loss and grief and mourning. We’ve been writing about it for as long as we’ve had written language. What strikes me, though, watching so many people experiencing loss, is that it is always hard. Losing a loved one is hard. It does not matter if your father is 50 or 90. It does not matter if your mothe

A Novel Approach to AF Ablation
A few short words about our conversation: Two decades have passed and electrophysiologists have learned little about how to ablate atrial fibrillation. Now, and then, we simply ablate circles around the orifices of the pulmonary veins. This works reasonably well. But we don’t—exactly—know why it works. For instance, some patients have total elimination of AF, but when they are restudied, they have reconnection of PV activity. Observations like these suggest there is something else happening with our ablations—beyond building an electric fence around the veins.One possibility is that we are affecting the neural input to the heart. Structures called ganglionic plexi sit next to the areas we ablate. We often see heart rate increases after AF ablation. Say, from 60 to 80 bpm. That’s because ablation has reduced parasympathetic input to the heart. Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.Piotr and his team had to suspend typical AF ablation during the pandemic. Surgeons would not provide backup. This gave them the idea of a simple approach—only in the right atrium, with one catheter, and no anesthesia. It turns out that there is often a ganglionic plexus in the upper right atrium. They found patients who had a history of vagally-mediated AF. They documented that these patients had high vagal tone. And… in these patients, simple ablation in the RA yielded a signal of benefit, a reduction of AF. Wow. It’s a small single-center study. It’s just a signal. A first mile of a marathon. But for the curious regarding AF, it is super-interesting. Many athletes and young people have vagally-mediated AF. Here is the link to the paper: Cardioneuroablation of Right Anterior Ganglionated Plexus for Treatment of Vagally Mediated Paroxysmal Atrial FibrillationHere is Piotr. He works in Rzeszów, Poland. It’s a beautiful city to visit. I once ran a marathon there. JMM This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Video version of our podcast
We discuss the state of medical education, Harvard music video, causal language at JAMA and more This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Cifu, Mandrola, Prasad
Video will be available to paid subscribers This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

A Discussion with Dr. Dena Zeraatkar regarding analytic flexibility in observational studies
Gosh was this a great conversation about her recent paper on specification curve analysis of nutritional observational studies. Here is Dr. Zeraatkar’s bio:Dena Zeraatkar, PhD is an Assistant Professor in the Departments of Anesthesia and Health Research Methods, Evidence, and Impact (HEI) at McMaster University. She earned her doctoral degree at McMaster University in the Health Research Methodology graduate program. Following her doctoral training, she pursued postdoctoral training at Harvard Medical School, for which she was awarded a Banting scholarship.Her research centers on evidence synthesis and evaluation—identifying and appraising research to optimally inform healthcare and public health decisions. She often works in areas in which the evidence is complex or conflicting, examples of which include nutrition and COVID-19 therapeutics. For her research, in 2023, she was awarded a Gairdner Early Career Investigator Award.First, it would help to read my comments yesterday on the paper. Dr. Zeraatkar is well-spoken, clear and she explains a complicated topic in simple terms. Her work is exactly the type we love at Sensible Medicine. Stay for her final comment. It made me so happy. Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 38: Yesterday’s Solutions; Today’s Problems
The Thomas Sowell quote, “On closer scrutiny, it turns out that many of today's problems are a result of yesterday's solutions” has been ringing in my head a lot lately. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Yet Another Excellent Explainer About P-Values in Randomized Trials
Gosh was I lucky to speak with Professor Erik Van Zwet from Leiden University in the Netherlands. He is the first author on a recent NEJM Evidence paper looking at more than 23,000 trials in the Cochrane Database. (I linked to an URL that should get by the paywall.) There are technical aspects of this paper. We hit on some (not a lot) of them. The gist of it though is really important when we look at evidence. Erik did an excellent job of explaining P-values, trial power, and, at the end, we discuss how this work might inform the ability of trials to replicate. This discussion also pairs well with one I had with computer scientist Ben Recht. I hope you enjoy the conversation. Please do consider subscribing or supporting our work as Sensible Medicine remains an ad-free user-supported place to learn about medical evidence. JMM Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 37: Why I Teach (acceptable and less acceptable reasons)
Why have I been committed to medical education? Some of the reasons are admirable but not terribly novel. Others are a bit hard to admit, but just as true. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 36: Why Don’t Doctors Want to See Patients?
Friday Reflection 35: Why Don’t Doctors Want to See Patients?I was asked “Why is it that doctors don’t want to see patients?” and I could not answer the question. Fourteen months later, here is my response. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

New Austrian Study Shows Boosters do NOT reduce COVID19 deaths in people who had COVID
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Math Professor Ben Recht and I Discuss P-values and Confidence Intervals
Ben Recht is a professor at UC Berkeley. You know, the place that has all those parking spaces for the Nobel laureates. He understands the innards of math. And that is exactly why he explained that doctors who use evidence don’t have to get bogged down in technicalities. I reached out to Ben to discuss a complicated but provocative statistical paper in NEJM evidence. But we mostly talk basics. Ben writes at his Substack arg min This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe
A discussion with the primary investigator of the world's first placebo-controlled AF ablation trial
As many of you know, I have long argued (unsuccessfully until now) for a placebo-controlled trial of AF ablation. One group gets the ablation; the other gets a placebo or sham procedure. This way we can sort out the placebo-resistant effect of the ablation. Finally, here is the first report of one. Dr. Malcolm Finlay is an electrophysiologist at St Bartholomew hospital in London UK and primary investigator of the study. They recently published their feasibility study for AF ablation vs placebo. The American Heart Journal published the pilot study of 20 patients. Finlay and colleagues call it the ORBITA AF trial. But it’s important to note that this was done separate from the ORBITA investigators at Imperial College. The larger study will have a different name. Here is a copy and paste:Twenty patients with PersAF (duration The primary endpoint was to evaluate the blinding of the patients. The good news is that it mostly worked. Blinding was successful in most patients. Recurrence of AF was less in the ablation vs cardioversion arm. But the numbers were too small to say much. Same with quality of life measures, which were mostly similar until 12 months. The authors concluded that This feasibility study establishes the potential for conducting a blinded, placebo-controlled trial to evaluate the efficacy of PVI versus DCCV in patients with PersAF.I hope you enjoy the conversation. This is darn exciting for the field. And I am delighted to publish this conversation on Sensible Medicine. (I also tried to include the un-edited transcript of the conversation.)Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Mandrola and Prasad are back
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Mandrola and Prasad are back
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 35: Four Who Fired Me
These patients did the right thing leaving my care. We were wrong for each other, or I had given what I had to offer (at the time) and it was not enough. That does not lessen the feeling that I failed. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 32: The Trauma of Not Dying Alone
They say dying alone is sad. They also say we all die alone. There is trauma to not dying alone as well. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Soren Diederichsen on Atrial Fibrillation Screening
If you care about AF you will love this conversation. Soren has some interesting ideas about what AF is now vs what AF was in the past. Here are some links:The LOOP Study (which was non-significant). Effects of Atrial Fibrillation Screening According to N-Terminal Pro-B-Type Natriuretic Peptide: A Secondary Analysis of the Randomized LOOP StudySeverity and Etiology of Incident Stroke in Patients Screened for Atrial Fibrillation vs Usual Care and the Impact of Prior Stroke: A Post Hoc Analysis of the LOOP Randomized Clinical TrialSensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.BTW: This is the kind of content we aim to bring you at Sensible Medicine. Thanks for your support. I have some great ideas for future conversations. Feel free to let me know your interests, too. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe
Andrew Foy has a Different Conclusion on a Big JAMA paper on CV risk reduction
The study in question is a randomized clinical trial looking at the Million Hearts Model. This model paid health care organizations to assess and reduce CV risk. Obviously, this is an important goal. Heart disease, specifically, atherosclerotic vascular disease, is a leading killer of humans. Any reduction of heart disease should have a benefit on both a person and a population. But paying health systems to do specific things is a policy intervention. Even though a policy, like this one, makes sense, policies can have benefits and potential harms. (An example is the hospital readmissions reduction program (HRRP), which penalized hospitals for excess readmissions. This resulted in a fewer readmissions but it also associated with an increase in death rates in patients with heart failure.)Both Andrew and I were happy that the nudging of Million Hearts was studied The Trial and ProgramThis was a big pragmatic cluster randomized trial that ran over 4 years. More than 300 organizations were randomly assigned 1:1 to have the Million Hearts model or standard care. There were two parts of the model. First there was $10 for every patient who had their 10-year risk calculated with a risk equation. (ACC/AHA is a simple one you can do in 15 seconds with a smartphone.) Then CMS paid each organization $0, $5, or $10 PBPM for each high-risk beneficiary with an annual risk reassessment, with monthly payment amounts dependent on mean risk score change across all of the organization’s high-risk beneficiaries reassessed.Keep in mind that the only components of the risk calculation that are modifiable are cholesterol and blood pressure. (*smoking cessation for smokers). Foy pointed out that Million Hearts was in many ways an incentive system to nudge providers, who then may nudge patients, to take more BP and cholesterol medicine. Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.The authors chose two primary outcomes: one a MACE endpoint with MI, stroke, and TIA. The second primary was the same as the first, plus CV death. They originally planned to include only high-risk patients, but then added moderate-risk patients. This factored heavily in the results. Patients were mostly 75 year-olds, men-women split 2/3rds, 1/3rd. Outcomes were derived from claims data—which is messy when it comes to judging MIs and TIAs and specific causes of death. The Results:The first primary endpoint (MI, stroke, TIA) occurred at a rate of 14.8 per 1000 patient-years vs 17.0 per 1000 patient-years. The Hazard ratio came to 0.97 (90% CI - 0.93-1.0). The P-value was 0.09. (The authors had previously stipulated that the P threshold would be 0.10). The second primary, adding in CV death, was similar. A HR of 0.96 (90% CI 093-0.99) and a P = 0.02. These are positive results. But let’s look further. Drivers of the Results: The results were driven almost exclusively by moderate risk patients. Look at Table 3. Reductions in events rates were largest and significant statistically in the moderate-risk but not high-risk group. That is something we have emphasized here at Sensible Medicine. Even though you would think that high-risk patients have the most to gain, they also have more competing risks and perhaps more chance for treatment harm. Like so many other studies, the sweet spot for primary prevention seems to be in the moderate-risk group. Unintended Consequences: A second finding, noted by Andrew, was the highly significant increase in all-cause hospitalizations in the intervention group. These had the most significant p-values of the entire study. Other Limitations:The Million Hearts model randomization was offered to more than 500 organizations but only 342 accepted. This raises the question of generalizability. Were the 342 organizations special in some way? Another factor is that outcomes were modeled on a sample of events—not raw counts. The choice to use 90% confidence intervals rather than 95% confidence intervals and P thresholds of 0.1 rather than the more standard of 0.05 is a weakness. For instance, the first primary endpoint would have missed significance if this were evaluated in the usual fashion. I did not find a strong justification for this choice. Readers with statistical expertise, please weigh in. Our Conclusions: First, we were both happy that a policy was studied rather than just implemented because it made sense. This should serve as a model for future policy endeavors. Second, there did look to be a modest effect on reducing important outcomes. And, these were driven mostly be moderate-risk (not high-risk) patients. This argues for a heterogenous treatment effect based on co-morbidity. Third, the statistically significant increase in all-cause hospitalizations in the intervention arm suggests that more aggressive attempts at blood pressure and cholesterol levels may have risen the risk of off-target ill effects. In the end, Andrew felt lik

Friday Reflection 31: Senses, Memories, and Medicine
Friday Reflection 31: Senses, Memories, and MedicineMedical training introduced me to a whole menu of smells -- both diagnostic tools and reminders of times in my career. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Sudden cardiac death and arrhythmias in athletes
Sudden cardiac death due to ventricular rhythm disturbances are rare but highly public. It’s strange and curious because you don’t expect healthy athletes to suffer serious cardiac issues. Recently three prominent athletes have survived sudden cardiac death. Christian Erikson, a Danish soccer player, Damar Hamlin, an American football player and Bronny James, son of Lebron James. These high-profile cases have highlighted the issue of sudden cardiac death of athletes. Dr. Dorian has published extensively on this topic. We had a great conversation. I learned a lot and hope you will too. JMM Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.Here are three pertinent articles he has published—note the first is from NEJM. Landry CH, Allan KS, Connelly KA, Cunningham K, Morrison LJ, Dorian P; Rescu Investigators. Sudden Cardiac Arrest during Participation in Competitive Sports. N Engl J Med. 2017 Nov 16;377(20):1943-1953. doi: 10.1056/NEJMoa1615710. PMID: 29141175; PMCID: PMC5726886.Weissler Snir A, Connelly KA, Goodman JM, Dorian D, Dorian P. Exercise in hypertrophic cardiomyopathy: restrict or rethink. Am J Physiol Heart Circ Physiol. 2021 May 1;320(5):H2101-H2111. doi: 10.1152/ajpheart.00850.2020. Epub 2021 Mar 26. PMID: 33769918.Weissler-Snir A, Allan K, Cunningham K, Connelly KA, Lee DS, Spears DA, Rakowski H, Dorian P. Hypertrophic Cardiomyopathy-Related Sudden Cardiac Death in Young People in Ontario. Circulation. 2019 Nov 19;140(21):1706-1716. doi: 10.1161/CIRCULATIONAHA.119.040271. Epub 2019 Oct 21. PMID: 31630535. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Prasad's lecture gets cancelled/ Cifu Gets COVID
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe
New Podcast -- Discussion with Rita Redberg and Angela Lu regarding Their Study on Conflict of Interest
Angela Lu is training to be a physician. She’s interested in public policy. As a third year medical student, she teamed up with established leaders to ask a unique question regarding public disclosure of financial relationships. When the Centers for Medicare & Medicaid Services (CMS) issues National Coverage Determinations (NCDs) for services or products, they mean business. Such decisions have huge implications. You cannot go against them. Think #HighConsequences.CMS studies the evidence and publishes a proposed decision. It then allows public comments. People care. The idea behind their study, which made it into the Journal of the American Medical Association, was to study how many commenters disclosed their financial conflicts. Dr. Lu went through more than 680 comments submitted on 4 NCDs—all of which were high cost invasive procedures. I won’t spoil the conversation, but they found a very high percentages of comments asking to expand indications for these procedures and very very low percentages of people who disclosed their relevant relationships. This study was made possible by the Open Payments database. One important note: disclosure of relationships was voluntary. Enjoy the conversation. Thanks for listening. JMM This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe
Foy and Mandrola Talk Coronary Calcium and a New Super-Exciting Approach to Medical Education
Andrew Foy rejoins the Sensible Medicine podcast. We talk first about coronary artery calcium. Andrew is an expert in this area. We have co-written our case against CAC scoring for any cause in the American Family Physician. It’s had little effect as CAC scoring is running rampant. Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.The second part of our conversation centers on a big med-ed project Andrew is co-leading at Penn State. He calls it Argue-to-Learn. The idea is to expose pre-clinical students to the value of civil debate. Here is their paper: Student Perceptions of a New Course Using Argumentation in Medical EducationHere is a quote: The absence of argumentation (i.e., a productive exchange of opposing views aimed at improved understanding of a given issue) in medical education may leave physicians susceptible to medical marketing, and incapable of both resolving industry claims and adapting to changing paradigms.Gosh. Gosh. Double Gosh, this is an exciting effort. Listen to Andrew explain. JMM This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Foy and Mandrola Discuss AF, AF-Ablation, Sham-controls, Evidence Translation and Heterogenous Treatment Effects
This week, I talk with Andrew Foy, who is an academic cardiologist at Penn State University in Hershey, PA. Andrew is one of the smartest voices in medicine today. We start with the REMEDIAL trial, published recently in JAMA. Ablation vs Meds. Primary endpoint—depression and anxiety. One of the main issues was the control arm—namely that there was no sham control. We referenced this useful review paper on placebo and nocebo effects in cardiology, from Brian Olshansky. Our second topic was the FRAIL AF trial. This was frail, elderly patients who had AF and were stable on Vitamin K antagonists (similar to warfarin) were randomized to remain on the VKA or switch to a direct acting oral anticoagulant. Primary endpoint—major bleeding. FRAIL AF is in Andrew’s wheelhouse as one of his primary academic areas of study is the role of multi-morbidity in translating medical evidence. He mentions a term called heterogenous treatment effects or HTE. I don’t love the term because it’s heavy into jargon. But HTE is super important for using evidence in the clinic. Andrew explains it well.Here is the editorial Andrew co-authored regarding another important trial in elderly patients who were having NSTEMI. I have written about FRAIL AF on Medscape and Sensible Medicine. We were going to talk about coronary artery calcium screening, but we had talked enough and will do a separate podcast on CAC. Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.As always, let us know what you think. We appreciate the support. Thank you. JMM This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Coumadin beats DOAC, ECMO fails, When RCTs needed, Bad COVID Policy
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 29: The Totally Predictable Doctor as Patient Essay
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Sensible Medicine x Vaccine Curious: Tracy Beth Høeg and Christine Stabell Benn compare US & Danish COVID-19 response and child vaccination policy
Sensible MedicineSensible Medicine x Vaccine Curious Cross Podcast on the USA vs Denmark, vaccines, etc:Show notes by Dovid Y Rimmer, Tracy Beth Høeg and Christine Stabell Benn* Benn, Høeg. Regarding becoming a medical skeptic. Hoeg: anonymous blog - exercise during pregnancy. Benn: Vitamins, sex differences, and vaccines.* Differences in pandemic response between Denmark v. California - school reopening, masks.* USA recommends boosters (yearly) for Children, Denmark does not recommend vaccinating children * Benn: Op-ed recommending gradual herd immunity.* Høeg, Duriseti, Prasad NEJM letter: Observational data for Covid mortality in vaccinated + boosted population (Source the original study, raw data release in response to letter, and Prasad NEJM letter).* Chandra & Høeg reanalysis of MMWR study: Differences in Covid-19 between schools mandating masks and not mandating. MMWR did not publish reanalysis, published in Journal of Infection.* Høeg et al reanalysis of Cowger et al. in NEJM, differences between schools mandating masks and not mandating in Boston, MA.* Six Clalit Health studies from Israel published in prestigious medical journals - the studies did not release their data or analyses to the public. (What were the points they made that influenced policy decisions, where were they cited, altimetric score. i.e. note that they were effective influencing policy without transparency).* Childhood vaccination schedules: Denmark 18 doses and USA 50 doses vaccination schedules. Note: differences regarding Influenza, Hep A & B, Varicella, Meningococcal, and Covid-19 which may be added to a yearly schedule. Denmark and Sweden don’t recommend yearly influenza vaccine in non high-risk under 65. * Denmark requires benefit for children, Finland allows societal considerations such as socioeconomic component of rotavirus. Finland uses influenza vaccine. And Denmark might introduce flu vaccine to reduce the flu burden on the elderly.* Ethics of consequentialist vaccine policy.* Pandemrix Swine flu vaccine had an adverse effect event of narcolepsy (hundreds of children affected), Denmark was spared some of the consequence by limiting its recommendation to vulnerable children only.* Flu deaths approximately 2-4/million, amongst children (Norway, US).* Nordic countries were hesitant to recommend routine Covid-19 vaccination. Denmark admits it was a mistake to recommend vaccinating children (it was done for the adults and since the vaccine was leaky it made no difference, everyone got it anyway).* Norway found in their pandemic investigation 6 weeks school closure was ‘a mistake’.Key academic claims:* Benn paper on Covid-19 becoming a childhood disease.https://www.bmj.com/content/374/bmj.n1687/rr-8 * Benn: Predictably Covid-19 would be dangerous only to old, vulnerable, and those with a large viral inoculum.https://pubmed.ncbi.nlm.nih.gov/32146445/ and https://pubmed.ncbi.nlm.nih.gov/6741923/ * Benn: Non-trivial C19 Death amongst elderly, but it probably didn’t change the amount of years they lived. https://pubmed.ncbi.nlm.nih.gov/33137809/ * The greater the inoculum the more harmful the disease. Example: measles index cases v. https://pubmed.ncbi.nlm.nih.gov/6741923/ * Covid-19 harms, are rare in children. Actual risk to children prior to natural immunity and afterward (Ideally include all risks, Death, hospitalization, severe disease). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9613797/, risks of severe disease https://pubmed.ncbi.nlm.nih.gov/35962242/ * Even rare harms would outweigh the benefits of widespread childhood vaccination. https://www.bmj.com/content/374/bmj.n1687/rr-8* Amongst most viruses the 2nd infection is less pathogenic.* Harms of lockdown exceeded benefits in quality studies, some non quality studies might indicate otherwise. https://www.tandfonline.com/doi/full/10.1080/00779954.2020.1844786?src=recsys, https://www.tandfonline.com/doi/abs/10.1080/13571516.2021.1976051 * Measles index cases (Child contracts the virus at school) results in more mild disease, family transmission is more severe with 4x fold mortality. https://pubmed.ncbi.nlm.nih.gov/6741923/ This has also been shown in animal studies https://pubmed.ncbi.nlm.nih.gov/36992457/. Epidemiological studies: Secondary cases (Family transmission) for Pertussis, https://pubmed.ncbi.nlm.nih.gov/11798255/ Varicella https://pubmed.ncbi.nlm.nih.gov/15702036/ and other viruses are worse than index cases i * Hoeg: MMWR School transmission of c19 is rare: https://www.cdc.gov/mmwr/volumes/70/wr/mm7004e3.htm This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 28: Four of the Things Patients Have Taught Me
Although it is unoriginal to point out that doctors learn from our patients, here are a few lessons so powerful, so extrapolatable, that I forever associate them with an individual. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Mandrola & Prasad on Republicans and COVID outcomes, Journals and stenting
This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

A Conversation with Professor Robert Yeh
Here is the profile for Harvard Professor Robert (Bobby) Yeh. His most recent Circulation paper: Bringing the Credibility Revolution to Observational Research in Cardiology. We referenced a paper by Professor Miguel Hernan: The C-Word: Scientific Euphemisms Do Not Improve Causal Inference From Observational DataPaper referenced on left ventricular assist devices: Comparative Effectiveness of Percutaneous Microaxial Left Ventricular Assist Device vs Intra-Aortic Balloon Pump or No Mechanical Circulatory Support in Patients With Cardiogenic ShockSensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.I learned a lot from this conversation. One of the main lessons is that no matter how well the authors avoid causal language, the intent of an observational comparison study is causal. And if that is so, the main thrust of these efforts ought to be simulate, as close as possible, a randomized clinical trial. One of my favorite parts of our chat was Bobby’s now famous explanation of immortal time bias using Cheetos. Let us know what you think. I hope to do more of these types of conversations. JMM This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Friday Reflection 27: The Poor Historian
BW was a 66-year-old woman who presented for an urgent visit to the general medicine clinic. She reported that she had been having dizziness for the last four days. When pressed, she said it occurred intermittently, being present more than absent. She could not identify any palliative or provocative features, and when asked about associated symptoms she said that she felt “bad and scared” when it was present. The doctor encouraged her, many times, to characterize the dizziness, and she could only say that when she had it, she felt dizzy.Sensible Medicine is a reader-supported publication. If you appreciate our work, consider becoming a free or paid subscriber.Many a medical trainee has been humiliated on morning rounds after proclaiming that their presentation was wanting because the “patient was a poor historian.” Any attending worth her white coat will respond in one of the following ways:“There are no poor historians, just poor history-takers.”“You do realize, don’t you, that the patient is not the historian? You are the historian.”“Did you consider the differential diagnosis of why you were unable to obtain a useful history?”I admit that, going for pith over constructive criticism, I employ the former two more than the latter one. There is a differential diagnosis for the patient who cannot describe the history of their medical concerns.Often, the inability of a doctor to obtain a history is actually a physical exam finding – an extremely non-specific finding, but a finding nonetheless. Psychiatric disease, dementia, and delirium (whose differential diagnosis itself is practically a textbook of medicine) will render a patient unable to provide an accurate history. I can recall dozens of “poor historians'' who became Robert Caro-esque once their hypercapnea, uremia, or alcohol withdrawal was treated.There are three other reasons that obtaining reliable and informative histories might be a struggle.1. We think with languageThe first — the saddest, most troublesome, and probably most common – reason that patients are unable to provide a reliable history is because of their impaired language skills. Not only do we use language to communicate, we also use language to think. George Orwell wrote, “…if thought corrupts language, language can also corrupt thought.”[i]Those of us who failed to master language, usually through inadequate education, are unable to express their health concerns clearly. Sometimes, listening to a patient try to describe symptoms, I get the sense that the problem is more than expressive.BW was not an especially striking example of this for me, she was just one of the more recent. She also presented with a problem for which an accurate history is critical. The history of a patient's dizziness radically alters the differential diagnosis. We teach trainees that the first question to pose to a patient with dizziness is, “What do you mean, dizzy?” We tell the trainee to ask the question and then sit back and listen. More often than not, patients will describe their dizziness in a way that can be interpreted as lightheadedness, vertigo, unsteadiness, or a non-specific feeling of being unwell.[ii]As I interviewed BW, my sense was that she not only struggled to articulate what she was feeling but to figure it out herself. Beyond my frustration in having trouble caring for her, I considered the lifelong impact of leaving people educationally impoverished. Sure, we limit people’s earning potential, but we also limit their internal life and their healthcare.2. Anxiety affects how we experience symptomsVG is a patient I have seen for years, from his mid 30’s to his early 60’s. He has a few very mild chronic medical conditions and very severe anxiety disorder. He is a successful professional but struggles with intermittent episodes of health-related anxiety.Our interactions usually begin with an email or a phone call. VG will have become anxious about a new symptom. The symptom is real – joint pain, a rash, a new floater. The symptom has generated a web of worry about what it could portend. The worries are always baseless and would be amusing if they were not so clearly painful and disturbing to him.I have learned that for VG, as well as for many patients like him, these concerns require a visit. An accurate history cannot be obtained without seeing him. The anxiety clouds VG’s experience of the symptom. The knee pain becomes excruciating, the rash ubiquitous, the floater debilitating. The response to simple questions -- Is the knee pain worse coming down the stairs? Where is the rash? Do you see the floater in one or both eyes? -- become unreliable. Seeing VG, providing some reassurance, and obtaining objective physical data is imperative.3. Secondary gain“Listen to your patient; he is telling you the diagnosis” is is an Osler (or merely Oslerian) quotation. From the earliest days of our training we are taught to listen to our patients and believe what they are telling us. Our greatest sin in hist

Friday Reflection #26: General Internal Medicine in the Time of COVID
There is something valuable about learning to adapt old skills to novel situations. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe

Podcast discussion on Nutrition Science, HFpEF and the NYT article on treatment of PAD
Adam and I discuss three topics I) The MIND Trial published in NEJM. Does a special diet reduce the future risk of cognitive decline?II) HFpEF — I am speaking at a congress on heart failure with preserved ejection fraction this week, and Adam helps me out with some pointers. III) NYT published a Sunday front page story on potential overuse of procedures for peripheral artery disease. JMM This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe