
EMplify by EB Medicine
315 episodes — Page 3 of 7
Conversations - Dr. Lorna Breen Legislation
Conversations - Dr. Lorna Breen Legislation
Episode 68 -- Meningitis and Encephalitis – An Interview with Dr. Andrew Hogan
Episode 68 -- Meningitis and Encephalitis – An Interview with Dr. Andrew Hogan
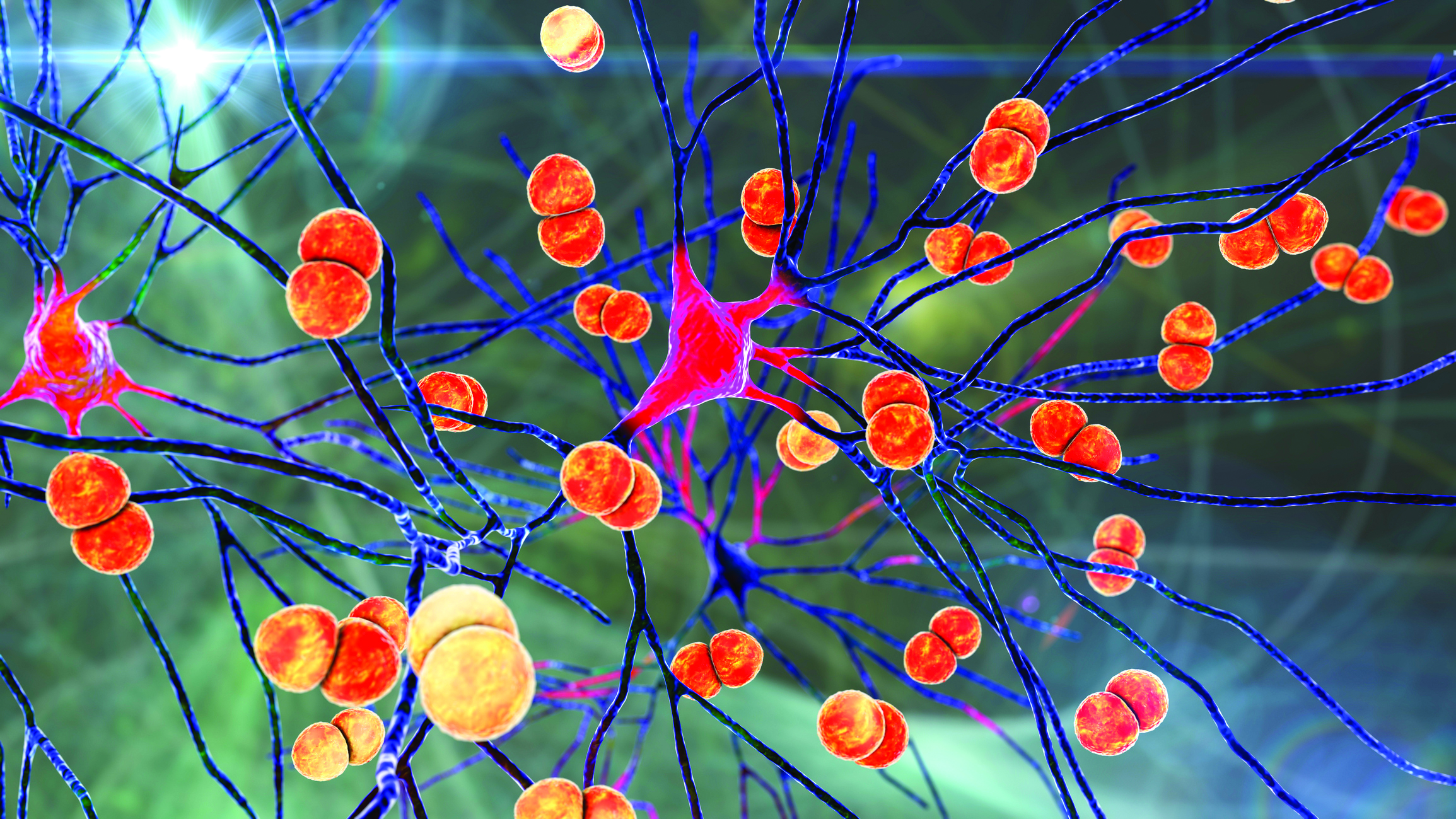
Episode 68 -- Meningitis and Encephalitis – An Interview with Dr. Andrew Hogan
Episode 68 -- Emergency Department Management of Adults With Infectious Meningitis and Encephalitis – An Interview with Dr. Andrew HoganEMplify -- April 2022Interview with the Author: Andrew N. Hogan, MD1.Meningitis vs encephalitisWhy this topic?What do the words mean? What's the difference?2.Bacterial meningitisHow common is it in the US? Is it more common in third world countries?Mortality rate in the USCauses – if Neisseria and H influenzae improved post vaccination, why not S pneumoniae disease ? (Table 1)3.Viral meningitisHow common is it in the US?What are the common causes? (Table 2)4.Viral encephalitisSame prognosis as viral meningitis?Same organisms as viral meningitis? (Table 2)Does COVID-19 cause this illness?5.Fungal infectionsWho gets these?60% die? 1 million cases a year, 600K deaths?6.Prehospital care:What does EMS need to know?How do they protect themselves from being exposed?How can they help us make the diagnosis?EMS is giving antibiotics in some areas?PEP7.ED evaluation: History8.ED evaluation: Physical exam9.Diagnostics: CSFWhat's large volume? Is it safe?Cell counts on tubes 1+4, all the time or only if traumatic and obviously bloody?Is opening pressure helpful?CSF lactate level – can this be run in a normal lactic acid analyzer?PCR/NAAT testing10.Serum labsWhat is helpful?Serum PCRSerum cryptococcal antigen11.Imaging Is CT imaging before LP still necessary? Can we be selective?Is MRI helpful in the ED, or is there a role in encephalitis?12.TreatmentAntibioticsSteroids: Who gets them? When? Are there downsides of giving them?13.Special populationsAutoimmune diseaseLacking childhood vaccinesHealthcare associated infections14.Cutting edge15.Disposition
Episode 67 – Managing Postpartum Complications in the Emergency Department – An Interview with Dr. Nicole Yuzuk, Dr. Joseph Bove, and Dr. Riddhi Desai
Episode 67 – Managing Postpartum Complications in the Emergency Department – An Interview with Dr. Nicole Yuzuk, Dr. Joseph Bove, and Dr. Riddhi Desai

Episode 67 – Managing Postpartum Complications in the Emergency Department – An Interview with Dr. Nicole Yuzuk, Dr. Joseph Bove, and Dr. Riddhi Desai
Episode 67 – Managing Postpartum Complications in the Emergency Department – An Interview with Dr. Nicole Yuzuk, Dr. Joseph Bove, and Dr. Riddhi DesaiEMplify – March 2022Interview with the Authors: Nicole Yuzuk, DO, Joseph Bove, DO, and Riddhi Desai, DOEpisode Outline:1.Why is this an important topic in EM? 2.Hemorrhage etiologies and definition3.Headache etiologies, both common and the more dangerous (ICH)4.Fever and infectionMastitisEndometritis5.Preeclampsia/eclampsia Definition, diagnosis, risk factors (Table 1)6.HELLP syndromeDefinition, diagnosis (Table 2)7.Peripartum cardiomyopathyTime of onset, how to make the diagnosis, risks (Table 3)8.Prehospital careIV fluidsTXAAMS evaluationChest painFever/hypotension 9.ED evaluation History (what kind of things should we remember to ask?) Physical exam (what should we be paying attention to?) 10.Diagnostic studiesHemorrhage (exam, vitals, labs, US)Headache (labs, imaging – what type?)Fever and infection (labs, imaging – US or CT, antibiotics)Cardiopulmonary complaints (labs, imaging, ECG)11.TreatmentHemorrhage Headache (CVT)Infection (mastitis, endometritis, wound Infection)Preeclampsia, eclampsia, HELLP, seizuresCardiomyopathy12.What about breastfeeding mothers? 13.Controversies and cutting edgeEndovascular therapyThromboelastography

Episode 66 - Acute Asthma
Episode 66 – Acute Asthma Exacerbations – An Interview with Dr. Steven Hochman and Dr. Brandon SomwaruEMplify – February 2022Emergency Department Management of Acute Asthma ExacerbationsInterview with the authors: Steven M. Hochman, MD, and Brandon Somwaru, DO Episode Outline:EpidemiologyRisk factors for death from asthma (Table 1)Triggers for asthma attacksVariants of asthma (Table 2)Differential diagnosis (Table 3)Can PE be a trigger for an acute asthma attack? Prehospital careED care: history (what should we ask?)ED care: physical exam (what are we looking for?)Classifying mild/moderate/severe asthma Lab studiesPOCUS (Table 5 and Figure 3)Peak expiratory flowETCO2 capnography and capnometryChest x-rayTreatment (Table 6)MedicationsOxygenSABA vs LABAWhat about MDIs?Continuous nebs?AnticholinergicsSteroids (IV, oral, inhaled; prednisone vs dexamethasone)Magnesium sulfateEpinephrineTerbutalineKetamineNIPPVIntubation pearls and pitfalls (Table 8)Special populationsPediatrics PregnancyCOVID-19 Controversies and cutting edgeBiologicsFractional exhaled nitric oxideHeliox High flow nasal cannulaDelayed sequence intubationECMODisposition
Episode 66 - Acute Asthma
Episode 66 - Acute Asthma
Episode 65 – Acute Joint Pain
Episode 65 – Acute Joint Pain
Episode 65 – Acute Joint Pain
Interview with author: Rachel Sullivan, MDWhy joint pain ?Differential Diagnosis Mono vs Poly Articular Presentation? Figure 1Infectious, degenerative, autoimmune, crystal deposition, reactive, traumaticSeptic Arthritis-Bimodal incidence RisksSeptic arthritis is polyarticular in 15% to 20% of cases, and in these cases, the mortality is highGonococcal Highest riskCommonly affected jointsSymptomatic or asymptomatic infection Lyme ArthritisViral – Zika, chikungunya, human parvovirus B19, hepatitisDegenerative osteoarthritis AutoimmuneGoutCPPDPrehospital ED History – table 2, table 4ED exam Labs – do we need them? ImagingArthrocentesis – Table 5TreatmentSpecial PopulationsProstheses Immunocompromised HIVClinical Pathway
Episode 64 – Thoracic Aortic Syndromes- An Interview with Dr. Anthony Hackett
Episode 64 – Thoracic Aortic Syndromes- An Interview with Dr. Anthony Hackett
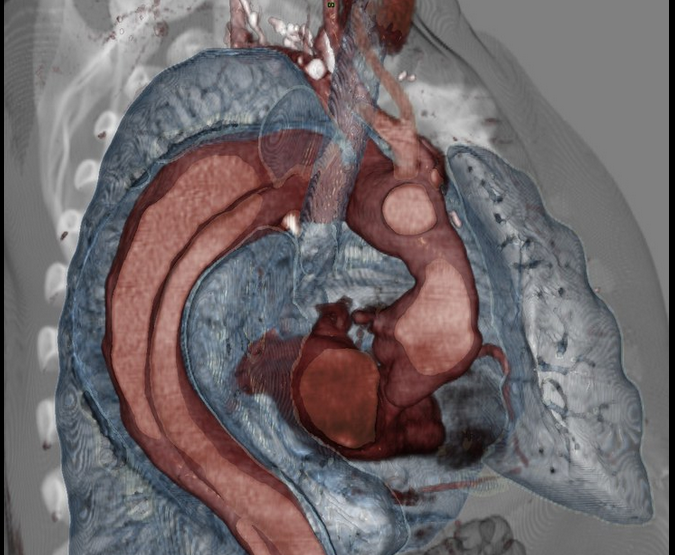
Episode 64 – Thoracic Aortic Syndromes- An Interview with Dr. Anthony Hackett
EMplify – December 2021Announcements:The EB Medicine app is live and available for free in the Apple Store. Coming to Google Play soon. It is in Beta and your feedback is welcome. ,This month get a $50 Amazon Gift Card with all orders over $300 at https://www.ebmedicine.netCheck out the newly redesigned FOAMed blog at https://www.ebmedicine.net/ebmblog/Thoracic Aortic Syndromes in The Emergency Department: Recognition and ManagementInterview with author: Anthony Hackett, MDThoracic Aortic SyndromesDissection, Intramural Hematoma, and Penetrating Aortic UlcersPathophysiologyIntima, media, and adventitiaEpidemiology and classification Debakey vs Stanford classification- do we still use Debakey ? Risk FactorsPrehospital Care – what should EMS be looking for? ED CareHistory HTN, Pulse defecits, Chest Pain, Syncope?Table 3ADD-RS scoreExamDiagnosticsLabsEKG – STEMI? ImagingCXREcho CTMRIAortogramTreatmentBP managementHeart RateShockSurgery – Who goes and when? Special populationsPregnancyControversiesD-Dimer
Episode 63 – Rib Fracture- An Interview with Dr. Patrick Maher
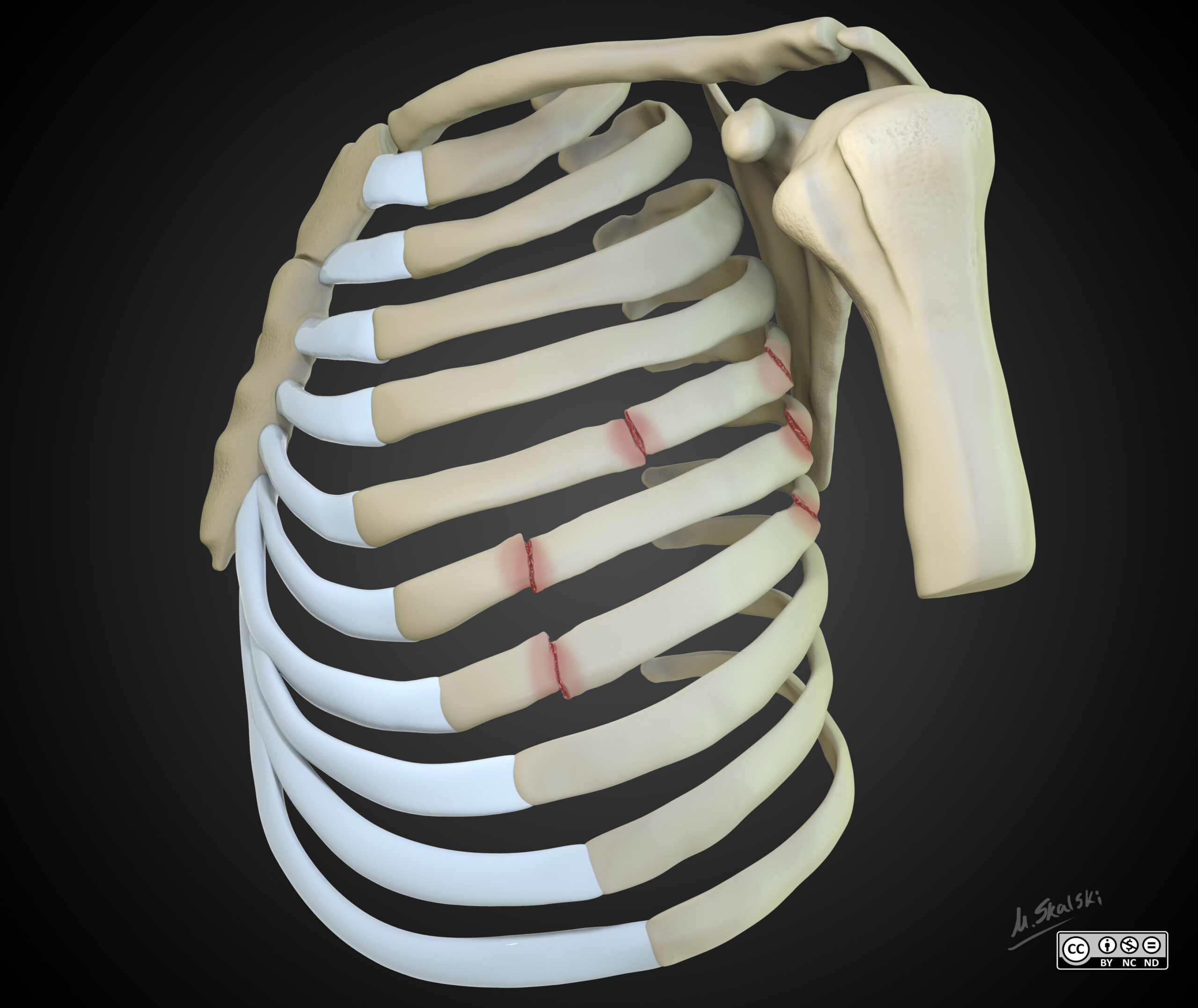
Episode 63 – Rib Fracture- An Interview with Dr. Patrick Maher
EMplify – November 2021Announcements:The EB Medicine app is live and available for free in the Apple Store. Coming to Google Play soon. It is in Beta and your feedback is welcome. ,Also, this month use code ACEP21! and get 20% of all orders at https://www.ebmedicine.netEmergency Department Management of Rib FracturesAuthor: Patrick Maher, MDEpisode Outline:Why rib fractures?AnatomyFig 1Pre-hospitalED evaluationHistory Physical ExamImagingNexus Chest Decision Instrument in Blunt TraumaACR criteria for imagingCT vs xrayUltrasound TreatmentMedsBindersKinesiotaping – Fig 4Respiratory supportOperative fixationSpecial PopulationsElderlyCancer patientsPediatricsDispositionBattle ScoreRib ScoreFVC
Episode 63 – Rib Fracture- An Interview with Dr. Patrick Maher

Episode 62 - Cervical Spine Injuries- An Interview with Dr. Jara-Alamonte
EMplify - October 2021Announcements: The EB Medicine app is live and available for free in the Apple Store. Coming to Google Play soon. It is in Beta and your feedback is welcome. ,Also, this month use code SB25 and get a $25 Starbucks gift card when you subscribe at ebmedicine.net Emergency Dept. Management of Cervical Spine Injuries Authors: Geoffrey Jara-Alamonte, MDChandni Pawar, MDEpidemiologyAnatomy (Figure 2 +3)Spinal Cord Injury Injury (Table1)PrimarySecondaryDifferential DiagnosisPrehospital Care - selective immobilizationED evaluationsHistoryPhysical Exam (Table 6)ImagingVascular Injury - Modified Denver Criteria (table 9)TreatmentSpecial PopulationsPediatrics
Episode 62 - Cervical Spine Injuries- An Interview with Dr. Jara-Alamonte
Episode 62 - Cervical Spine Injuries- An Interview with Dr. Jara-Alamonte
Episode 61 - Abnormal Uterine Bleeding
Episode 61 - Abnormal Uterine Bleeding
Episode 61 - Abnormal Uterine Bleeding
EMplify - September 2021Announcements: Be on the lookout for an announcement regarding the new EB Medicine app, coming to an App Store near you this month !! Also, this month use code SB25 and get a $25 Starbucks gift card when you subscribe at ebmedicine.net !Abnormal Uterine Bleeding in the Emergency DepartmentAuthors:Tazeen Abbas, MDAbbas Husain, MD, FACEPPhysiology reviewTerminologyDifferentiating Causes: PALM-COEINStructural: Polyp, Adenomyosis, Leiomyoma, Malignancy/HyperplasiaNon-structural: Coagulopathy, Ovulatory dysfunction, Endometrial, Iatrogenic, Not otherwise specifiedOther causes: thyroid disease, hyperprolactinemia, stress, weight loss and anorexia, heavy exerciseAge Based Differential12-18Immaturity of the hypothalamic-pituitary- ovarian axisSexually transmitted infectionsCoagulopathies, and bleeding disorders (von Willibrand disease)19-39polypsfibroidsmalignancyPCOSAge 40 and olderendometrial atrophymalignancyHistoryPhysical ExamDiagnostic StudiesTreatmentUnstableStableSpecial CasesDOACsPrepubescent girlsgenital injuries

Episode 60 – Less Lethal Law Enforcement Weapons
EMplify – August 2021Announcements: Be on the lookout for an announcement regarding the new EB Medicine app, coming to an App Store near you this month !!August 2021 Pediatric Emergency Medicine PracticeLess Lethal Law Enforcement WeaponsAuthors: Jessica Osterman, MD , Cara Buchanan, MDWhat kinds of less-lethal weapons are law enforcement using?Pepper sprayConducted Electrical Weapons (CEWs)K-9sBeanbag gunsRubber bulletsStingballsDifferential DiagnosisPrehospital CareTrauma Informed CareConductive Electrical Weapons – TaserChemical Irritants- Pepper Spray, Tear GasK9 InjuriesKinetic Impact Projectiles- Rubber Bullets, Beanbags, Sting Balls/GrenadesSounds:Police Siren https://freesound.org/people/MultiMax2121/sounds/156869/Ambulance https://freesound.org/people/sofialomba/sounds/469413/Angry Man https://freesound.org/people/ebcrosby/sounds/334439/Taser https://freesound.org/people/The_Chemical_Workshop/sounds/403252/Taser https://freesound.org/people/Greub/sounds/402636Coughs https://freesound.org/people/freesound/sounds/25301/Dog Bark https://freesound.org/people/ivolipa/sounds/337101/Grenade https://freesound.org/people/superfreq/sounds/268101/Last Updated on April 29, 2022
Episode 60 – Less Lethal Law Enforcement Weapons
Episode 60 – Less Lethal Law Enforcement Weapons
Episode 59 – HIV – An Interview With Dr. Daniel Egan
Episode 59 – HIV – An Interview With Dr. Daniel Egan
Episode 59 – HIV – An Interview With Dr. Daniel Egan
EMplify – July 2021Announcements: Be on the lookout for an announcement regarding the new EB Medicine app, coming to an App Store near you this month !!HIV- An Interview With Dr. Daniel EganSee the EB Medicine Article @ https://www.ebmedicine.net/topics/infectious-disease/HIVWhy HIV? 2018 , 1,2 million people living with HIV, almost 40k new infectionsPeople living with HIV visit the ED 3 x per year on averageHIV infected patients accounted for 6 in 1000 ED visits in 2017New Transmission of HIV, Figure 1What does acute infection look like ?What about chronic infection ?The chronic phase can last 10 years or more and be asymptomatic.Are people with HIV more likely to develop: CAD, COPD, DVT and why?What if they are on medication for HIV?Screening in the ED, everyone? Do they have to have symptoms or risks?What does universal screening mean?What does risk based screening mean?What are the risk factors? What if I see someone on PrEP who is in the ED for an unrelated complaint?HistoryAsk about cd4 and viral load and last testAsk about he of opportunistic infectionsAsk about medication side effectsWhat else?ExamLabs – rapid testing, 4th gen, viral load and cd4, etcImagingTreatmentTable 1Highly effective and reduces transmissionMedication side effects (we don’t have to dwell on each Med and side effect and just reference the charts)hep B virus deactivationSystem Based DiseaseHeart Failure and CADPCP (role of LDH)TBCOPDRenal Disease – stones , radiolucentNeurologic- CVA, cryptococcal meningitis, toxo, progressive multi focal leukoencephalopathy, HANDGI – diarrhea causes, c diff, hep CHeme- cytopeniaEndocrine – metabolic syndromeMusculoskeletalPsychiatric table 3DermSpecial CircumstancesPEPPrEP
Episode 58 – Syncope – An Interview With Dr. James Morris

Episode 58 – Syncope – An Interview With Dr. James Morris
EMplify - June 2021 Announcements: The Clinical Decision Making in the Emergency Department conference is June 23-27 live and virtual. More information here: https://clinicaldecisionmaking.com Be on the lookout for an announcement regarding the new EB Medicine app, coming to an App Store near you this summer !! Syncope- An Interview With Dr. James Morris See the EB Medicine Article @ https://www.ebmedicine.net/topics/cardiovascular/syncope Why syncope? Prevalence, hospitalizations, etc. Etiology: figure 1 is fantastic. Physiologic basis of syncope Neurally mediated Orthostatic - are we still doing orthostatic vitals in the ED? Cardiac Differentiating syncope from seizure Features that point to seizure Urinary incontinence Number of jerks Age? Prehospital care is all about details What did bystanders see? What do paramedics see? Any trauma? Any neuro deficits ? Glucose ECG ED History - table 4 History of similar Prodrome Associated symptoms (chest pain, neuro symptoms, etc) Falls Pre-syncope ? ED exam Vitals, vitals, vitals Orthostatic vitals ? Carotid sinus massage, why this? Do we do in the ED? ECG Brugada, blocks, VT, ST changes, etc Labs BNP, delta bnp ? Trop Lactic acid Pregnancy test CBC lutes Bun/Cr Echo - any role in the ED? CT Head PE- get this on everyone ? Is it high prevalence? Risk stratification tools- the bad and the worse Table 7, amazing Controversies Admitting the elderly Orthostatic vitals (we discussed already) Disposition
Episode 58 – Syncope – An Interview With Dr. James Morris
Episode 57 – Atrial Fibrillation : An Approach To Diagnosis And Management In The Emergency Department
EMplify - May 2021 Announcements: The Clinical Decision Making in the Emergency Department conference is June 23-27 live and virtual. More information here: https://clinicaldecisionmaking.com Be on the lookout for an announcement regarding the new EB Medicine app, coming to an App Store near you this summer !! Atrial Fibrillation : An Approach To Diagnosis And Management In The Emergency Department - An Interview with Dr Brian Millman Epidemiology Causes Prehospital treatment - careful with causes of the A Fib. ED Evaluation History - beware the causes Physical ECG Labs Imaging Echocardiography Treatment Rate control Calcium channel blockers Beta blockers Esmolol Magnesium Rhythm control Amiodarone Procainamide Cardioversion Watch and Wait Anticoagulation Disoposition
Episode 57 – Atrial Fibrillation : An Approach To Diagnosis And Management In The Emergency Department
Episode 57 – Atrial Fibrillation : An Approach To Diagnosis And Management In The Emergency Department
Episode 56 - Management of Suspected Rabies Exposure in the Emergency Department
Episode 56 - Management of Suspected Rabies Exposure in the Emergency Department

Episode 56 - Management of Suspected Rabies Exposure in the Emergency Department
EMplify - April 2021AnnouncementsTraumatic Hemorrhage in the ED- with Dr Scott Weingart - April 13th, 8pm EST Free ! Register now: https://www.crowdcast.io/e/traumatic-hemorrhagic/registerPandemic Preparedness publication is coming soon.Mt Sinai COVID-19 Treatment Protocols have been updated and are available for free here: https://www.ebmedicine.net/topics/COVID-19/ProtocolsThe Clinical Decision Making in the Emergency Department conference is June 23-27 live and virtual. More information here: https://clinicaldecisionmaking.com Management of Suspected Rabies Exposure in the Emergency Department - An Interview with Dr. Bess StorchEpidemiology:Fatality rate of over 99%Half of cases occur in children95% of cases are in resource limited countries, 35% in India99% caused by infected dogs (worldwide)In the US, cases are predominantly bat variantWhy this topic?"In a recent survey of licensed physicians, less than half could identify rabies transmission routes, the correct PEP schedule, and the correct anatomic administration sites."Pathophysiology:What causes it? The RNA virus LyssavirusHow is it transmitted?How does it reach the brain?ED Evaluation:What does it look like clinically?5 stages- incubation, prodrome, acute neurologic phase, coma deathWhy doesn’t everyone just get vaccinated?What patient medical history is important ? Steroids, chloroquineWhat animals are high risk?What about pets and quarantine?What about rodents ?Is there any role for labs or imaging ?What is the treatment regimen for those who are unvaccinated? And vaccinated?What about people who are immunosuppressed?Children?Pregnant?Recently traveled?
Episode 55 -Management of Acute Urinary Retention in the Emergency Department
Episode 55 -Management of Acute Urinary Retention in the Emergency Department

Episode 55 -Management of Acute Urinary Retention in the Emergency Department
EMplify - March 2021Management of Acute Urinary Retention in the Emergency Department An algorithmic approach to urinary retention.Relieve the obstruction FoleyCudet catherSilicone catheterSuprapubic catheterDetermine the cause - StructuralMedications / ToxicologicNeurologicInfectiousAlpha blockersAntibioticsSlow vs rapid bladder decompressionAdmit or dischargePhimosis and ParaphimosisAnnouncements: New Airway Course Available: Current Topics in Airway Management: Mechanical Ventilation, Supraglottic Airway Devices, and Intubating Patients With COVID-19Upcoming Live Course: Dr. Scott Weingart - Traumatic Hemorrhage - April 13th., 8-9pm, ESTLook for the "Key Points And Pearls From 2020" coming to your inbox or mailbox next month !
Episode 54 - Community-Acquired Pneumonia in the Emergency Department - Interview with Matthew DeLaney, MD
Episode 54 - Community-Acquired Pneumonia in the Emergency Department - Interview with Matthew DeLaney, MD
Episode 54 - Community-Acquired Pneumonia in the Emergency Department - Interview with Matthew DeLaney, MD
EMplify - February 2021Community Acquired Pneumonia - An Interview with Dr. Matthew DeLaney, FACEP1. Pneumonia and nomenclature : healthcare associated vs hospital associated2. COVID-19 and antibiotics3. Bacteriology - Strep is only 10-15% of hospitalized pneumonia, Viral pneumonia is about 20% (pre covid)4. Conditions that predispose to pneumoniachronic lung disease (chronic obstructive pulmonary disease, bronchiectasis)smokingolder ageimmuno-compromiseproton-pump inhibitors, H2 blockers, and antipsychotic agents5. Is there a historical or exam item most likely to be indicative of pneumonia?6. How good is a CXR?7. When should I consider a CT if the CXR is normal?8. Procalcitonin9. Blood cultures, sputum cultures, urine antigens- are these helpful?10. CURB-65 vs PSI11. Antibiotics- table 3 major and minor, history of prior infection, and doxy for everyone !12. Duration - 5 days works13. A walk through the pathway
Episode 53- Evaluation and Management of ST-Segment Elevation Myocardial Infarction in the Emergency Department
Episode 53- Evaluation and Management of ST-Segment Elevation Myocardial Infarction in the Emergency Department
Episode 53- Evaluation and Management of ST-Segment Elevation Myocardial Infarction in the Emergency Department
EMplify January 2021Evaluation and Management of ST-Segment Elevation Myocardial Infarction in the Emergency DepartmentAuthorsMarshall Frank, DO, MPH, FACEPCarson Sanders, BS, NRP, CCEMT-PBryan P. Berry, MD, BCEM, FACEP TopicsEpidemiologyPathophysiologyPrehospital careEmergency Dept EvaluationHistoryPhysicalImagingLabsElectrocardiogramaVRPosterior LeadsLBBBSerial ECGsReciprocal ChangesPericarditis vs STEMITreatmentOxygenOpioidsAntiplatelet AgentsNitroglycerinBeta BlockersReperfusionPCIThrombolyticsDysrhythmiasAnticoagulantsTransfersSpecial CircumstancesGenderAgeCocaineHave questions or comments on the podcast? Write us at [email protected] .